

Scaffold design for bone regeneration
- PMID: 24730250
- PMCID: PMC3997175
- DOI: 10.1166/jnn.2014.9127
Scaffold design for bone regeneration
Abstract
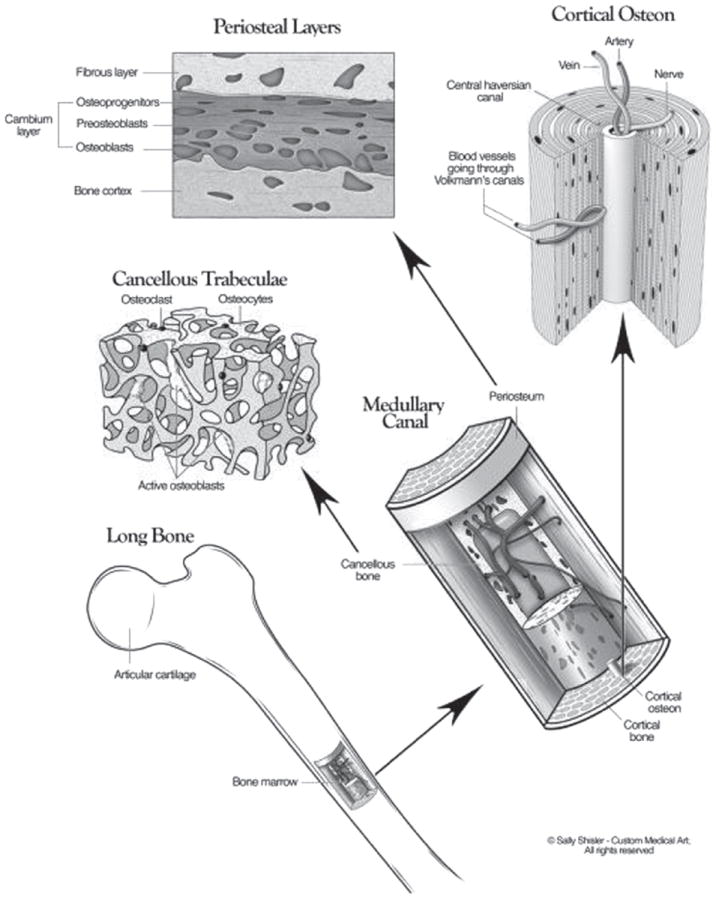
The use of bone grafts is the standard to treat skeletal fractures, or to replace and regenerate lost bone, as demonstrated by the large number of bone graft procedures performed worldwide. The most common of these is the autograft, however, its use can lead to complications such as pain, infection, scarring, blood loss, and donor-site morbidity. The alternative is allografts, but they lack the osteoactive capacity of autografts and carry the risk of carrying infectious agents or immune rejection. Other approaches, such as the bone graft substitutes, have focused on improving the efficacy of bone grafts or other scaffolds by incorporating bone progenitor cells and growth factors to stimulate cells. An ideal bone graft or scaffold should be made of biomaterials that imitate the structure and properties of natural bone ECM, include osteoprogenitor cells and provide all the necessary environmental cues found in natural bone. However, creating living tissue constructs that are structurally, functionally and mechanically comparable to the natural bone has been a challenge so far. This focus of this review is on the evolution of these scaffolds as bone graft substitutes in the process of recreating the bone tissue microenvironment, including biochemical and biophysical cues.
Figures
References
-
- Neighbour T. The Global Orthobiologics Market: Players, Products and Technologies Driving Change. Espicom Business Intelligence. 2008;2
-
- Brydone A, Meek D, Maclaine S. Proc Inst Mech Eng H. 2010;224:1329. - PubMed
-
- Myeroff C, Archdeacon M. J Bone Joint Surg Am. 2011;93:2227. - PubMed
-
- Oppenheim J, Segal D, Spitzer D. Neurosurgery. 2002;51:854. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical