

Effect of β-blockers on platelet aggregation: a systematic review and meta-analysis
- PMID: 24730697
- PMCID: PMC4243868
- DOI: 10.1111/bcp.12404
Effect of β-blockers on platelet aggregation: a systematic review and meta-analysis
Abstract
Aims: Platelets play an important role in cardiovascular disease, and β-blockers are often prescribed for cardiovascular disease prevention. β-Blockers may directly affect platelet aggregation, because β-adrenergic receptors are present on platelets. There is uncertainty about the existence and magnitude of an effect of β-blockers on platelet aggregation. The aim of this study was to perform a systematic review and meta-analysis of the effect of β-blockers on platelet aggregation.
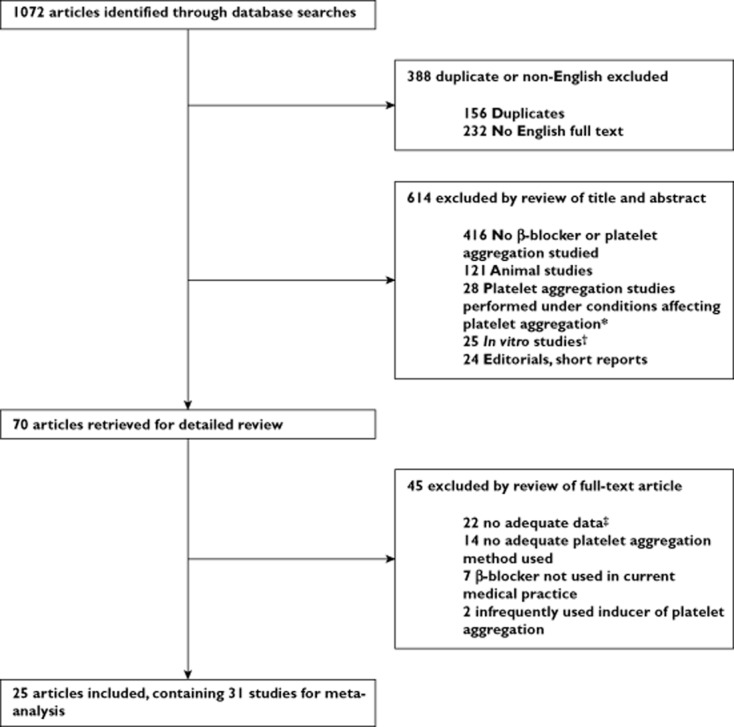
Methods: MEDLINE and EMBASE were searched until April 2014. Two reviewers independently performed data extraction and risk of bias assessment. Type of β-blocker, population, treatment duration and platelet aggregation were extracted. Standardized mean differences were calculated for each study and pooled in a random-effects meta-analysis.
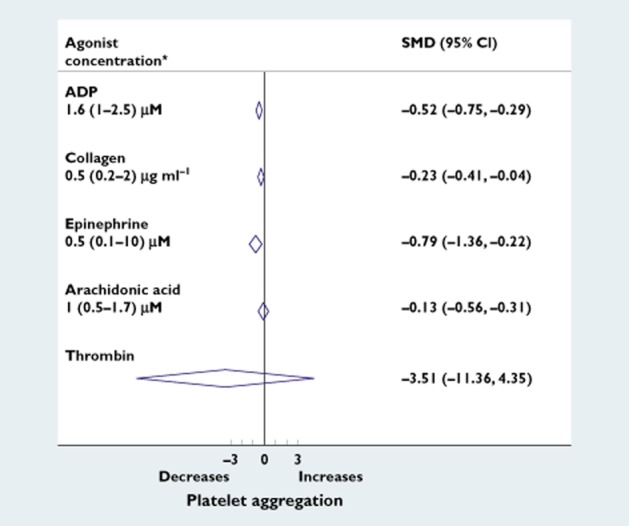
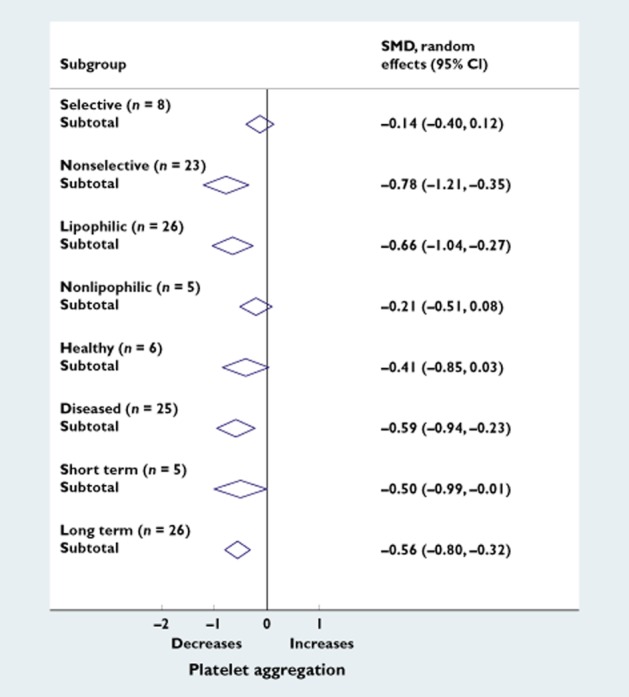
Results: We retrieved 31 studies (28 clinical trials and three observational studies). β-Blockers decreased platelet aggregation (standardized mean difference -0.54, 95% confidence interval -0.85 to -0.24, P < 0.0001). This corresponds to a reduction of 13% (95% confidence interval 8-17%). Nonselective lipophilic β-blockers decreased platelet aggregation more than selective nonlipophilic β-blockers.
Conclusions: Clinically used β-blockers significantly reduce platelet aggregation. Nonselective lipophilic β-blockers seem to reduce platelet aggregation more effectively than selective nonlipophilic β-blockers. These findings may help to explain why some β-blockers are more effective than others in preventing cardiovascular disease.
Keywords: meta-analysis; platelet aggregation; β-blockers.
© 2014 The British Pharmacological Society.
Figures

Comment in
-
Antiplatelet activity of β-blockers: new light on existing data.Br J Clin Pharmacol. 2014 Nov;78(5):937-9. doi: 10.1111/bcp.12438. Br J Clin Pharmacol. 2014. PMID: 24909390 Free PMC article. No abstract available.
References
-
- Nichols M, Townsend N, Scarborough P, Luengo-Fernandez R, Leal J, Gray A, Rayner M. 2012. European Cardiovascular Disease Statistics 2012. European Heart Network, European Society of Cardiology.
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics − 2012 update: a report from the American Heart Association. Circulation. 2012;125:e2–e220. - PMC - PubMed
-
- O'Gara PT, Kushner FG, Ascheim DD, Casey DE, Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX, Anderson JL, Jacobs AK, Halperin JL, Albert NM, Brindis RG, Creager MA, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Kushner FG, Ohman EM, Stevenson WG, Yancy CW. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362–425. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
