

Outcomes of men with an elevated prostate-specific antigen (PSA) level as their sole preoperative intermediate- or high-risk feature
- PMID: 24731026
- PMCID: PMC4352319
- DOI: 10.1111/bju.12771
Outcomes of men with an elevated prostate-specific antigen (PSA) level as their sole preoperative intermediate- or high-risk feature
Abstract
Objective: To investigate the post-prostatectomy and long-term outcomes of men presenting with an elevated pretreatment prostate-specific antigen (PSA) level (>10 ng/mL), but otherwise low-risk features (biopsy Gleason score ≤6 and clinical stage ≤T2a).
Patients and methods: PSA-incongruent intermediate-risk (PII) cases were defined as those patients with preoperative PSA >10 and ≤20 ng/mL but otherwise low-risk features, and PSA-incongruent high-risk (PIH) cases were defined as men with PSA >20 ng/mL but otherwise low-risk features. Our institutional radical prostatectomy database (1992-2012) was queried and the results were stratified into D'Amico low-, intermediate- and high risk, PSA-incongruent intermediate-risk and PSA-incongruent high-risk cases. Prostate cancer (PCa) features and outcomes were evaluated using appropriate comparative tests. Multivariable analyses were adjusted for age, race and year of surgery.
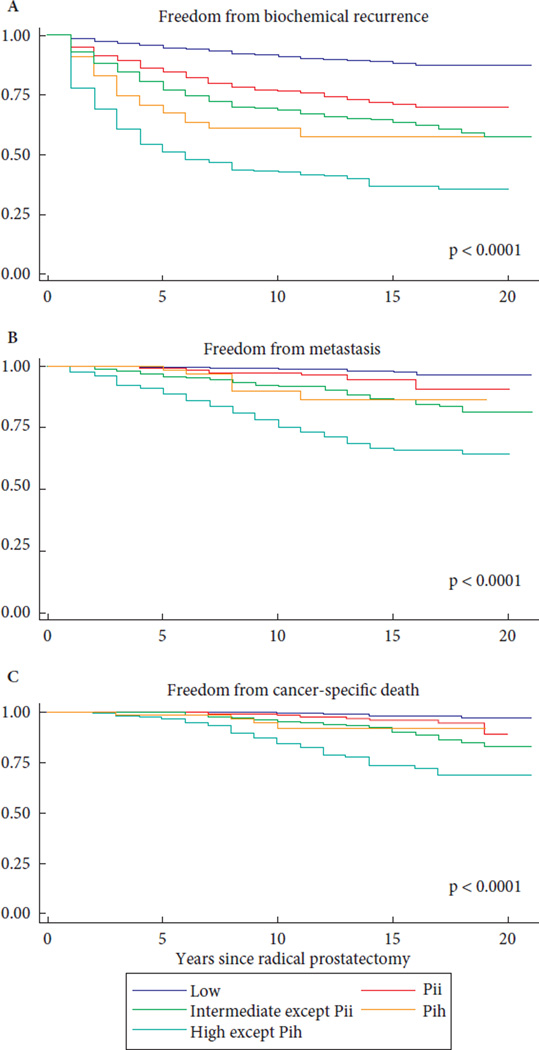
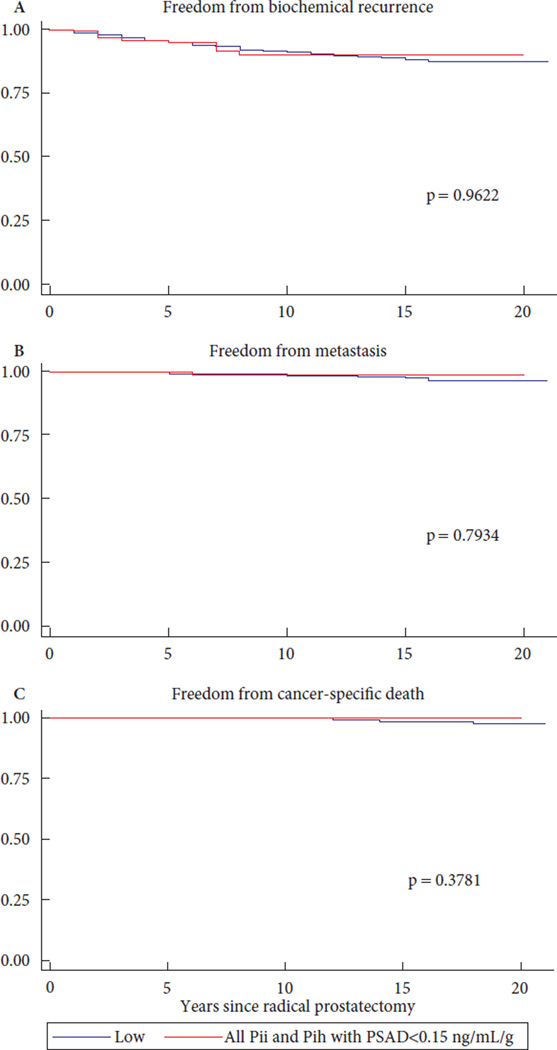
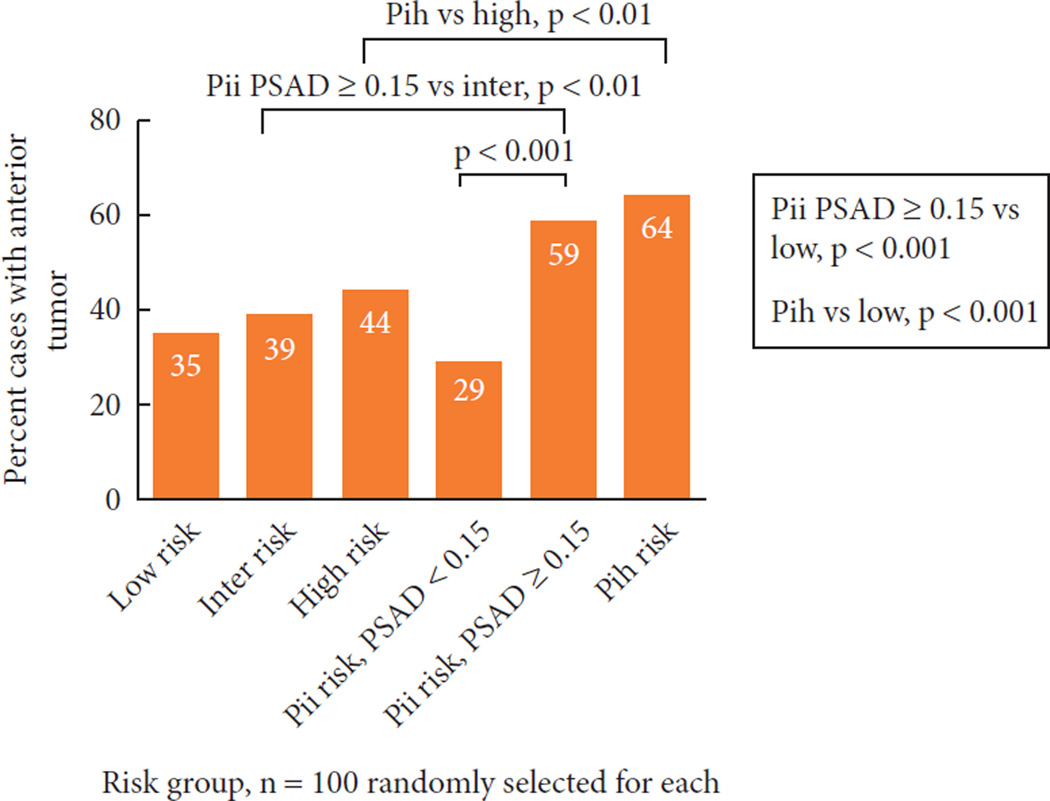
Results: Of the total cohort of 17 608 men, 1132 (6.4%) had PII-risk disease and 183 (1.0%) had PIH-risk disease. Compared with the low-risk group, the odds of upgrading at radical prostatectomy (RP) were 2.20 (95% CI 1.93-2.52; P < 0.001) for the PII group and 3.58 (95% CI 2.64-4.85; P < 0.001) for the PIH group, the odds of extraprostatic disease at RP were 2.35 (95% CI 2.05-2.68; P < 0.001) for the PII group and 6.68 (95% CI 4.89-9.15; P < 0.001) for the PIH group, and the odds of positive surgical margins were 1.97 (95% CI 1.67-2.33; P < 0.001) for the PII group and 3.54 (95% CI 2.50-4.95, P < 0.001) for the PIH group. Compared with low-risk disease, PII-risk disease was associated with a 2.85-, 2.99- and 3.32-fold greater risk of biochemical recurrence (BCR), metastasis and PCa-specific mortality, respectively, and PIH-risk disease was associated with a 5.32-, 6.14- and 7.07-fold greater risk of BCR, metastasis and PCa-specific mortality, respectively (P ≤ 0.001 for all comparisons). For the PII group, the higher risks of positive surgical margins, upgrading, upstaging and BCR were dependent on PSA density (PSAD): men in the PII group who had a PSAD <0.15 ng/mL/g were not at higher risk compared with those in the low-risk group. Men in the PII group with a PSAD ≥0.15 ng/mL/g and men in the PIH group were more likely to have an anterior component of the dominant tumour (59 and 64%, respectively) compared with those in the low- (35%) and intermediate-risk group (39%) and those in the PII-risk group with PSAD <0.15 ng/mL/g (29%).
Conclusions: Men with PSA >20 ng/mL or men with PSA >10 and ≤20 ng/mL with a PSAD ≥0.15 ng/mL/g, but otherwise low-risk PCa, are at greater risk of adverse pathological and oncological outcomes and may be inappropriate candidates for active surveillance. These men are at greater risk of having anterior tumours that are undersampled at biopsy, so if treatment is deferred, ancillary testing such as anterior zone sampling or magnetic resonance imaging should be strongly encouraged. Men with elevated PSA levels >10 and ≤20 ng/mL but low PSAD have outcomes similar to those in the low-risk group, and consideration of surveillance is appropriate in these cases.
Keywords: outcome; prostate cancer; prostate-specific antigen; prostatectomy; risk.
© 2014 The Authors. BJU International © 2014 BJU International.
Conflict of interest statement
Conflict of Interest
None declared.
Figures
Similar articles
-
The ability of prostate-specific antigen (PSA) density to predict an upgrade in Gleason score between initial prostate biopsy and prostatectomy diminishes with increasing tumour grade due to reduced PSA secretion per unit tumour volume.BJU Int. 2012 Jul;110(1):36-42. doi: 10.1111/j.1464-410X.2011.10681.x. Epub 2011 Nov 15. BJU Int. 2012. PMID: 22085203
-
Prostate-specific antigen density predicts extracapsular extension and increased risk of biochemical recurrence in patients with high-risk prostate cancer who underwent radical prostatectomy.Int J Clin Oncol. 2015 Feb;20(1):176-81. doi: 10.1007/s10147-014-0696-0. Epub 2014 Apr 29. Int J Clin Oncol. 2015. PMID: 24771079
-
Long-term cancer control outcomes in patients with clinically high-risk prostate cancer treated with robot-assisted radical prostatectomy: results from a multi-institutional study of 1100 patients.Eur Urol. 2015 Sep;68(3):497-505. doi: 10.1016/j.eururo.2015.06.020. Epub 2015 Jun 26. Eur Urol. 2015. PMID: 26119559
-
Prognostic Value of Biochemical Recurrence Following Treatment with Curative Intent for Prostate Cancer: A Systematic Review.Eur Urol. 2019 Jun;75(6):967-987. doi: 10.1016/j.eururo.2018.10.011. Epub 2018 Oct 17. Eur Urol. 2019. PMID: 30342843
-
Predictive Factors for Gleason Score Upgrading in Patients with Prostate Cancer after Radical Prostatectomy: A Systematic Review and Meta-Analysis.Urol Int. 2023;107(5):460-479. doi: 10.1159/000528873. Epub 2023 Mar 29. Urol Int. 2023. PMID: 36990065
Cited by
-
Predicting Gleason score using the initial serum total prostate-specific antigen in Black men with symptomatic prostate adenocarcinoma in Nigeria.Clin Interv Aging. 2016 Jul 18;11:961-6. doi: 10.2147/CIA.S98232. eCollection 2016. Clin Interv Aging. 2016. PMID: 27486316 Free PMC article.
-
Variation in serum prostate-specific antigen levels in men with prostate cancer managed with active surveillance.BJU Int. 2016 Oct;118(4):535-40. doi: 10.1111/bju.13328. Epub 2015 Oct 26. BJU Int. 2016. PMID: 26385021 Free PMC article.
-
Partial prostatectomy: technically feasible, but patient selection is paramount.Transl Androl Urol. 2017 Apr;6(2):308-309. doi: 10.21037/tau.2017.01.17. Transl Androl Urol. 2017. PMID: 28540241 Free PMC article. No abstract available.
-
Clinicopathologic characteristics of anterior prostate cancer (APC), including correlation with previous biopsy pathology.Med Oncol. 2015 Nov;32(11):249. doi: 10.1007/s12032-015-0693-9. Epub 2015 Oct 6. Med Oncol. 2015. PMID: 26442515
-
Active surveillance for intermediate-risk prostate cancer.Prostate Cancer Prostatic Dis. 2017 Mar;20(1):1-6. doi: 10.1038/pcan.2016.51. Epub 2016 Nov 1. Prostate Cancer Prostatic Dis. 2017. PMID: 27801900 Free PMC article. Review.
References
-
- D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280:969–974. - PubMed
-
- D’Amico AV, Cote K, Loffredo M, et al. Pretreatment predictors of time to cancer specific death after prostate specific antigen failure. J Urol. 2003;169:1320–1324. - PubMed
-
- Walz J, Joniau S, Chun FK, et al. Pathological results and rates of treatment failure in high-risk prostate cancer patients after radical prostatectomy. BJU Int. 2010;107:765–770. - PubMed
-
- D’Amico AV, Chen MH, Catalona WJ, et al. Prostate cancer-specific mortality after radical prostatectomy or external beam radiation therapy in men with 1 or more high-risk factors. Cancer. 2007;110:56–61. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
