

Patterns of surgical care and complications in elderly adults
- PMID: 24731176
- PMCID: PMC4024102
- DOI: 10.1111/jgs.12794
Patterns of surgical care and complications in elderly adults
Abstract
Objectives: To determine whether procedures, hospitals visited, and complications would differ according to decade in elderly adults and from those of younger adults.
Design: Retrospective cohort study.
Setting: The Anesthesia Quality Institute National Anesthesia Clinical Outcomes Registry (NACOR) is the largest database of anesthesia cases from academic and community hospitals and includes all insurance and facility types across the United States.
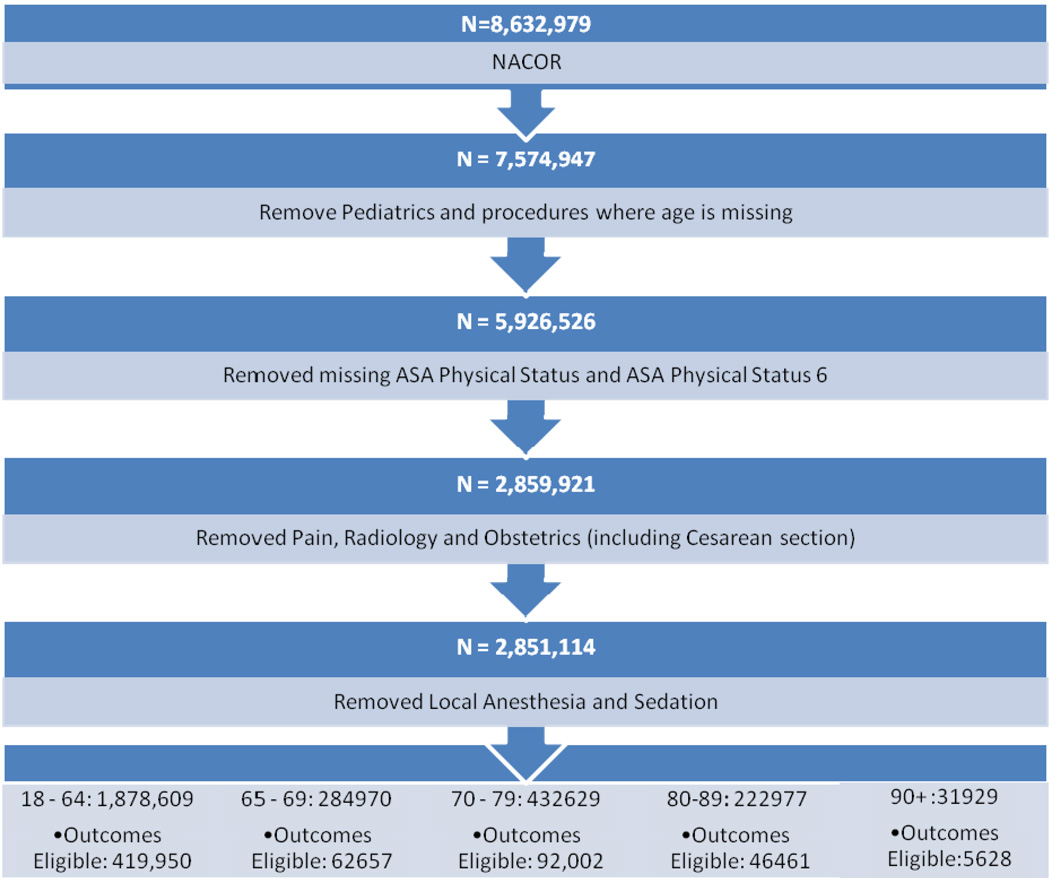
Participants: Eight million six hundred thirty-two thousand nine hundred seventy-nine cases from January 2010 to March 2013 were acquired. After exclusion of individuals younger than 18, nonapplicable locations, and brain death, 2,851,114 remained and were placed into age categories (18-64, 65-69, 70-79, 80-89, ≥ 90).
Measurements: Participant, surgical, anesthetic, and hospital descriptors and short-term outcomes (major complications, mortality at <48 hours).
Results: The largest number of older adults had surgery in medium-sized community hospitals. The oldest age group (≥ 90) underwent the smallest range of procedures; hip fracture, hip replacement, and cataract procedures accounted for more than 35% of all surgeries. Younger old adults underwent these procedures plus a significant proportion of spinal fusion, cholecystectomy, and knee surgery. Older adults had greater mortality and more complications than younger adults. Participants undergoing exploratory laparotomy had the greatest likelihood of death in any age category except 90 and older, in which small bowel resection predominated. The proportion of emergency surgery and the mortality associated with emergency surgery was 30% higher in the oldest group (≥ 90) than in adults aged 18 to 64.
Conclusion: This article reports the pattern of surgical procedures, complications, and mortality found in NACOR, which is one of the few data sets that contains data from community hospitals and individuals with all types of insurance. Because the outcomes portion of the data set is under development, it is not possible to investigate the relationship between hospital type and complications or mortality, but this study underscores the magnitude of geriatric surgery that occurs in community hospitals as an area for future outcomes studies.
Keywords: anesthesia; mortality; outcomes; surgery.
© 2014, Copyright the Authors Journal compilation © 2014, The American Geriatrics Society.
Conflict of interest statement
Stacie Deiner: Has NIH, FAER, AGS funding, and has served as an expert witness
Benjamin Westlake: works for the ASA AQI
Richard P. Dutton: works for ASA AQI, AQI board, expert witness
Figures
Comment in
-
Re: Patterns of surgical care and complications in elderly adults.J Urol. 2015 Apr;193(4):1290. doi: 10.1016/j.juro.2015.01.044. Epub 2015 Jan 19. J Urol. 2015. PMID: 25890526 No abstract available.
References
-
- The elderly population [Internet].: U.S. Census Bureau. Available from: http://eresources.library.mssm.edu:2114/population/www/pop-profile/elder....
-
- Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Rep. 2009;11:1–25. - PubMed
-
- Leung JM, Dzankic S. Relative importance of preoperative health status versus intraoperative factors in predicting postoperative adverse outcomes in geriatric surgical patients. J Am Geriatr Soc. 2001;49:1080–1085. - PubMed
-
- Garibaldi RA, Britt MR, Coleman ML, et al. Risk factors for postoperative pneumonia. Am J Med. 1981;70:677–680. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
