

Extended negative pressure wound therapy-assisted dermatotraction for the closure of large open fasciotomy wounds in necrotizing fasciitis patients
- PMID: 24731449
- PMCID: PMC3996171
- DOI: 10.1186/1749-7922-9-29
Extended negative pressure wound therapy-assisted dermatotraction for the closure of large open fasciotomy wounds in necrotizing fasciitis patients
Abstract
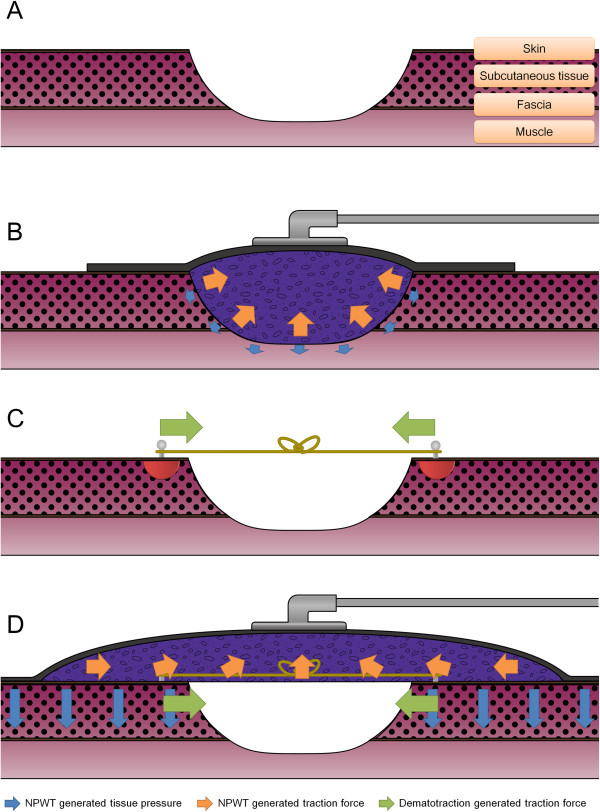
Background: Necrotizing fasciitis (NF) is a rapid progressive infection of the subcutaneous tissue or fascia and may result in large open wounds. The surgical options to cover these wounds are often limited by the patient condition and result in suboptimal functional and cosmetic wound coverage. Dermatotraction can restore the function and appearance of the fasciotomy wound and is less invasive in patients with comorbidities. However, dermatotraction for scarred, stiff NF fasciotomy wounds is often ineffective, resulting in skin necrosis. The authors use extended negative pressure wound therapy (NPWT) as an assist in dermatotraction to close open NF fasciotomy wounds. The authors present the clinical results, followed by a discussion of the clinical basis of extended NPWT-assisted dermatotraction.
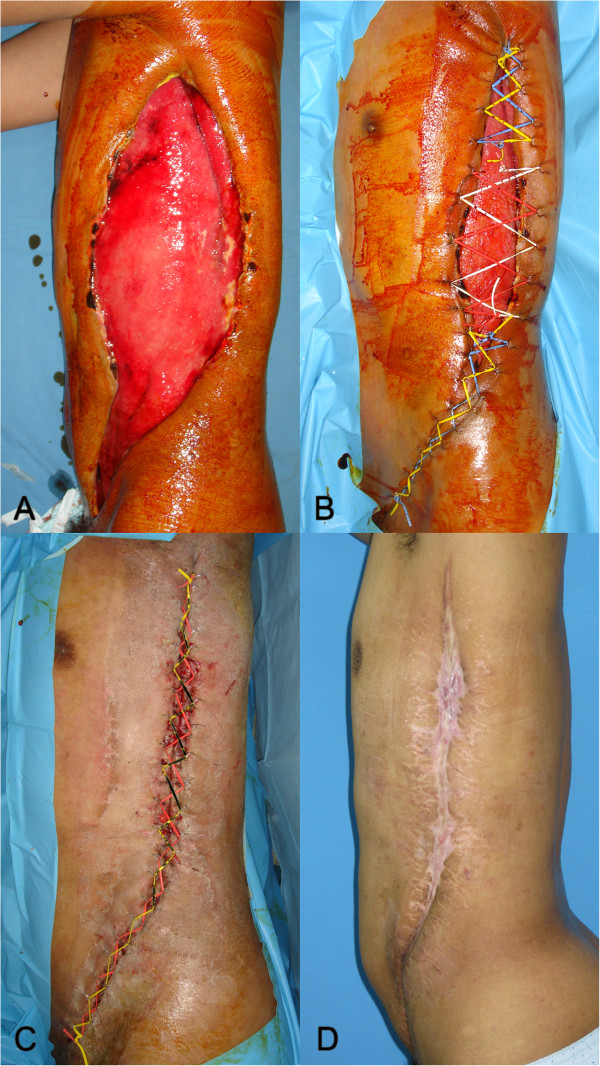
Methods: A retrospective case series of eight patients with NF who underwent open fasciotomy was approved for the study. After serial wound preparation, dermatotraction was applied in a shoelace manner using elastic vessel loops. Next, the extended NPWT was applied over the wound. The sponge was three times wider than the wound width, and the transparent covering drape almost encircled the anatomical wound area. The negative pressure of the NPWT was set at a continuous 100 mmHg by suction barometer. The clinical outcome was assessed based on wound area reduction after treatment and by the achievement of direct wound closure.
Results: After the first set of extended NPWT-assisted dermatotraction procedures, the mean wound area was significantly decreased (658.12 cm(2) to 29.37 cm(2); p = 0.002), as five out of eight patients achieved direct wound closure. One patient with a chest wall defect underwent latissimus dorsi musculocutaneous flap coverage, with primary closure of the donor site. Two Fournier's gangrene patients underwent multiple sets of treatment and finally achieved secondary wound closure with skin grafts. The patients were followed up for 18.3 months on average and showed satisfactory results without wound recurrence.
Conclusions: Extended NPWT-assisted dermatotraction advances scarred, stiff fasciotomy wound margins synergistically in NF and allows direct closure of the wound without complications. This method can be another good treatment option for the NF patient with large open wounds whose general condition is unsuitable for extensive reconstructive surgery.
Keywords: Dermatotraction; Fasciotomy; Fournier’s gangrene; Necrotizing fasciitis; Negative pressure wound therapy.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources
