

The polygenic nature of hypertriglyceridaemia: implications for definition, diagnosis, and management
- PMID: 24731657
- PMCID: PMC4201123
- DOI: 10.1016/S2213-8587(13)70191-8
The polygenic nature of hypertriglyceridaemia: implications for definition, diagnosis, and management
Abstract
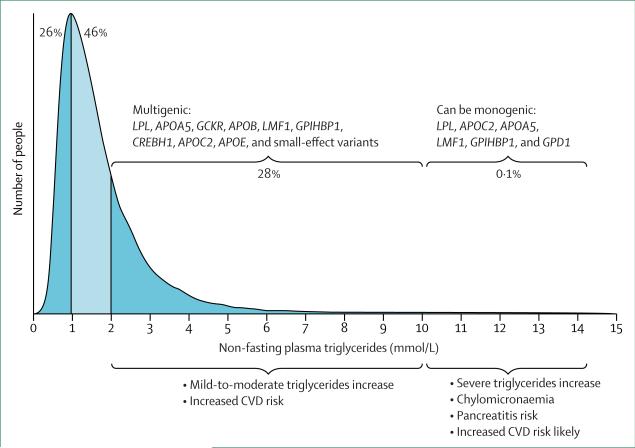
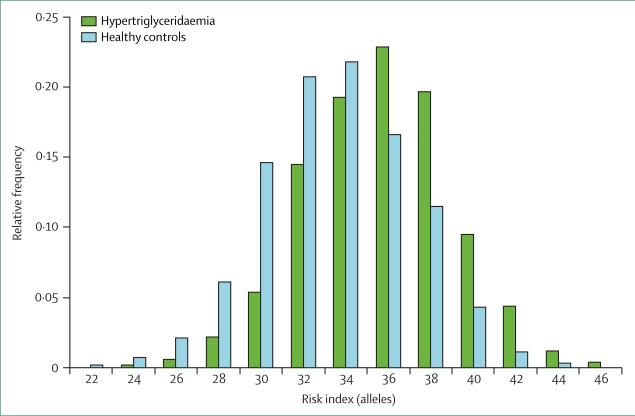
Plasma triglyceride concentration is a biomarker for circulating triglyceride-rich lipoproteins and their metabolic remnants. Common mild-to-moderate hypertriglyceridaemia is typically multigenic, and results from the cumulative burden of common and rare variants in more than 30 genes, as quantified by genetic risk scores. Rare autosomal recessive monogenic hypertriglyceridaemia can result from large-effect mutations in six different genes. Hypertriglyceridaemia is exacerbated by non-genetic factors. On the basis of recent genetic data, we redefine the disorder into two states: severe (triglyceride concentration >10 mmol/L), which is more likely to have a monogenic cause; and mild-to-moderate (triglyceride concentration 2-10 mmol/L). Because of clustering of susceptibility alleles and secondary factors in families, biochemical screening and counselling for family members is essential, but routine genetic testing is not warranted. Treatment includes management of lifestyle and secondary factors, and pharmacotherapy. In severe hypertriglyceridaemia, intervention is indicated because of pancreatitis risk; in mild-to-moderate hypertriglyceridaemia, intervention can be indicated to prevent cardiovascular disease, dependent on triglyceride concentration, concomitant lipoprotein disturbances, and overall cardiovascular risk.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Treatment of severe hypertriglyceridaemia.Lancet Diabetes Endocrinol. 2014 Nov;2(11):860. doi: 10.1016/S2213-8587(14)70052-X. Epub 2014 Mar 20. Lancet Diabetes Endocrinol. 2014. PMID: 25439459 No abstract available.
-
Treatment of severe hypertriglyceridaemia--authors' reply.Lancet Diabetes Endocrinol. 2014 Nov;2(11):860-1. doi: 10.1016/S2213-8587(14)70054-3. Epub 2014 Mar 20. Lancet Diabetes Endocrinol. 2014. PMID: 25439460 No abstract available.
References
-
- Boullart AC, de Graaf J, Stalenhoef AF. Serum triglycerides and risk of cardiovascular disease. Biochim Biophys Acta. 2012;1821:867–75. - PubMed
-
- Chapman MJ, Ginsberg HN, Amarenco P, et al. the European Atherosclerosis Society Consensus Panel Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: evidence and guidance for management. Eur Heart J. 2011;32:1345–61. - PMC - PubMed
-
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA. 2001;285:2486–97. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
