

Endocrine consequences of anorexia nervosa
- PMID: 24731664
- PMCID: PMC4133106
- DOI: 10.1016/S2213-8587(13)70180-3
Endocrine consequences of anorexia nervosa
Abstract
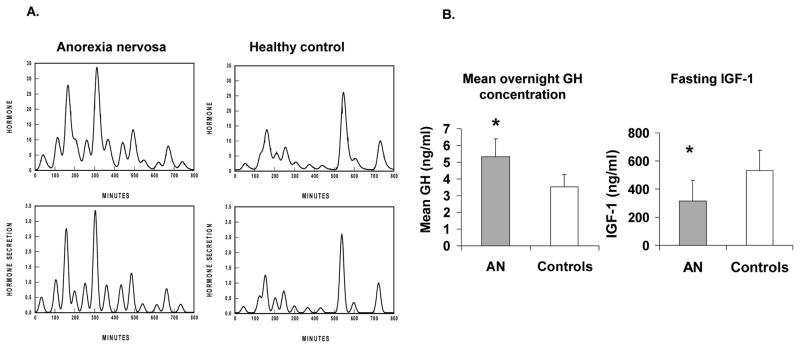
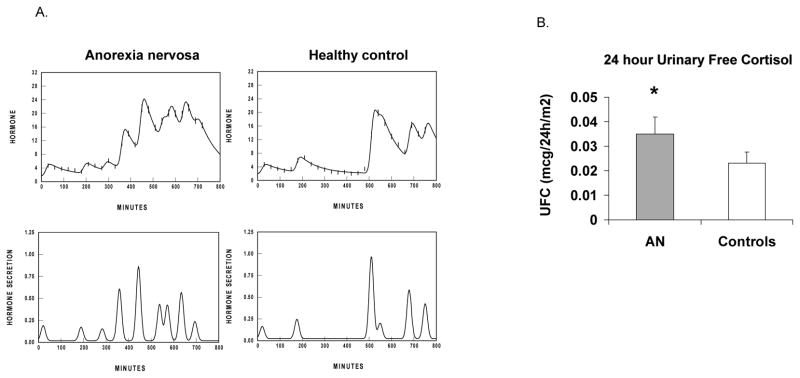
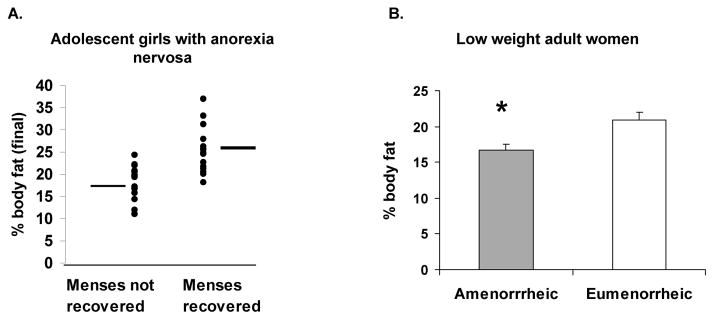
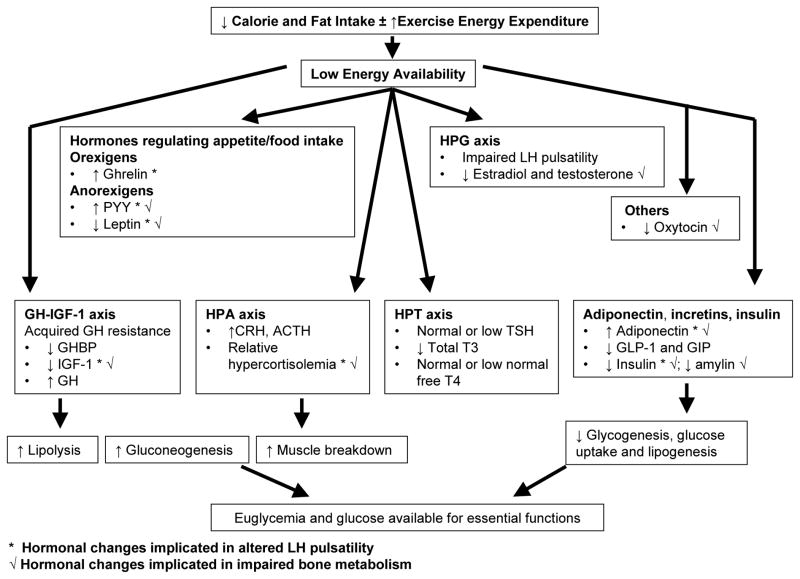
Anorexia nervosa is prevalent in adolescents and young adults, and endocrine changes include hypothalamic amenorrhoea; a nutritionally acquired growth-hormone resistance leading to low concentrations of insulin-like growth factor-1 (IGF-1); relative hypercortisolaemia; decreases in leptin, insulin, amylin, and incretins; and increases in ghrelin, peptide YY, and adiponectin. These changes in turn have harmful effects on bone and might affect neurocognition, anxiety, depression, and the psychopathology of anorexia nervosa. Low bone-mineral density (BMD) is particularly concerning, because it is associated with changes in bone microarchitecture, strength, and clinical fractures. Recovery leads to improvements in many--but not all--hormonal changes, and deficits in bone accrual can persist. Oestrogen-replacement therapy, primarily via the transdermal route, increases BMD in adolescents, although catch-up is incomplete. In adults, oral oestrogen--combined with recombinant human IGF-1 in one study and bisphosphonates in another--increased BMD, but not to the normal range. More studies are necessary to investigate the optimum therapeutic approach in patients with, or recovering from, anorexia nervosa.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to report
Figures


References
-
- Jaite C, Hoffmann F, Glaeske G, Bachmann CJ. Prevalence, comorbidities and outpatient treatment of anorexia and bulimia nervosa in German children and adolescents. Eat Weight Disord. 2013;18(2):157–65. - PubMed
-
- Wade TD, Bergin JL, Tiggemann M, Bulik CM, Fairburn CG. Prevalence and long-term course of lifetime eating disorders in an adult Australian twin cohort. Aust N Z J Psychiatry. 2006;40(2):121–8. - PubMed
-
- Pelaez Fernandez MA, Labrador FJ, Raich RM. Prevalence of eating disorders among adolescent and young adult scholastic population in the region of Madrid (Spain) J Psychosom Res. 2007;62(6):681–90. - PubMed
-
- Hoek HW. Incidence, prevalence and mortality of anorexia nervosa and other eating disorders. Curr Opin Psychiatry. 2006;19(4):389–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
