

Ultrasound-guided instrumental removal of the retained placenta after vaginal delivery
- PMID: 24732003
- PMCID: PMC4207252
- DOI: 10.1016/j.ajog.2014.04.012
Ultrasound-guided instrumental removal of the retained placenta after vaginal delivery
Abstract
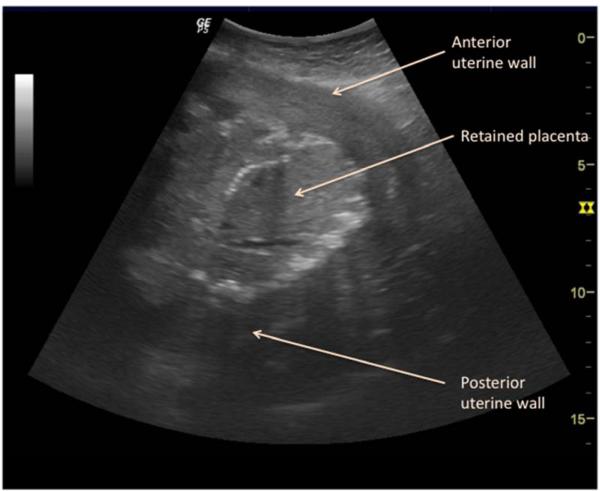
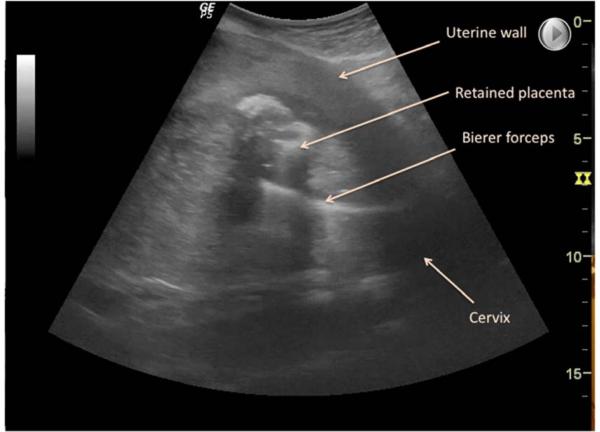
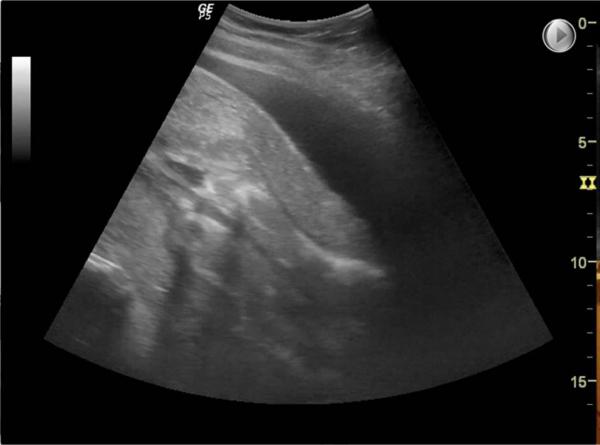
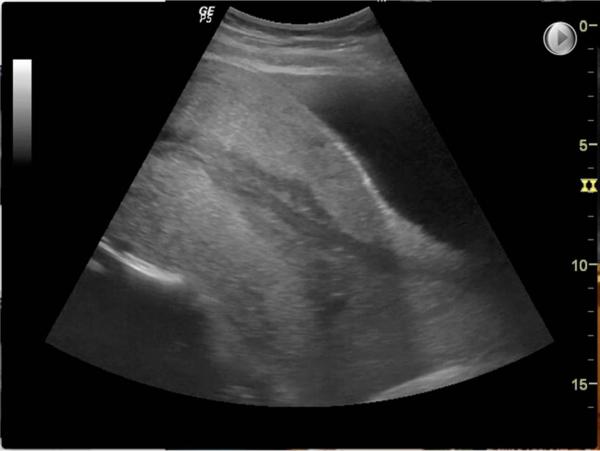
The standard treatment for retained placenta is manual extraction, in which a hand is introduced inside the uterus to cleave a plane between the placenta and the uterine wall. For women without an epidural, the procedure is extremely uncomfortable and may require additional measures such as intravenous narcotics or regional anesthesia. Although ultrasound-guided instrumental removal of the placenta is standard practice as part of second-trimester abortion by dilation and evacuation and may be done at many institutions, especially after failed manual extraction, it has not yet been described in the literature as a technique following vaginal birth. Our experience with this technique is that it causes less discomfort to the patient than a traditional manual extraction, because the instrument entering the uterus is much narrower than a hand. With the patient in dorsal lithotomy, we locate the cervix and stabilize it either with fingers or a ring forceps on the anterior lip. We introduce Bierer ovum forceps into the uterus under direct ultrasound guidance. The Bierer forceps are preferred because of their long length, large head, and serrated teeth that allow for a firm, secure grip on the placenta. We grasp the placental tissue with the forceps and apply slow, gentle traction in short strokes, regrasping increasingly more distal areas of placenta as necessary to tease out the placenta. After 1-2 minutes, the placenta separates and can be pulled out of the uterus, usually intact. Our experience suggests that this technique is a well-tolerated option for women without an epidural who have a retained placenta. Further study is needed to quantify the amount of discomfort and anesthesia that can be avoided with this technique, as well as whether there is any change in the frequency of infectious complications or the necessity of postremoval curettage.
Keywords: Bierer forceps; retained placenta; ultrasound guidance.
Copyright © 2014 Mosby, Inc. All rights reserved.
Figures

Similar articles
-
Immediate postpartum ultrasound evaluation for suspected retained placental tissue in patients undergoing manual removal of placenta.Eur J Obstet Gynecol Reprod Biol. 2015 Sep;192:37-40. doi: 10.1016/j.ejogrb.2015.06.004. Epub 2015 Jun 24. Eur J Obstet Gynecol Reprod Biol. 2015. PMID: 26149477
-
Predictive value of sonographic examination to visualize retained placenta directly after birth at 16 to 28 weeks.J Ultrasound Med. 2000 Jan;19(1):7-12; quiz 13-4. doi: 10.7863/jum.2000.19.1.7. J Ultrasound Med. 2000. PMID: 10625184
-
The role of ultrasound imaging in the management of partial placental retention after third trimester livebirth.J Matern Fetal Neonatal Med. 2022 Jun;35(11):2063-2069. doi: 10.1080/14767058.2020.1777272. Epub 2020 Jun 17. J Matern Fetal Neonatal Med. 2022. PMID: 32552068
-
Instrumental delivery: clinical practice guidelines from the French College of Gynaecologists and Obstetricians.Eur J Obstet Gynecol Reprod Biol. 2011 Nov;159(1):43-8. doi: 10.1016/j.ejogrb.2011.06.043. Epub 2011 Jul 28. Eur J Obstet Gynecol Reprod Biol. 2011. PMID: 21802193 Review.
-
[PROLONGED RETAINED PLACENTA ACCRETA IN THE UTERUS AFTER VAGINAL DELIVERY (A CASE REPORT AND REVIEW OF LITERATURE)].Akush Ginekol (Sofiia). 2015;54(3):34-9. Akush Ginekol (Sofiia). 2015. PMID: 26137778 Review. Bulgarian.
Cited by
-
Variety is the spice of life: new features in AJOG.Am J Obstet Gynecol. 2014 Sep;211(3):187-8. doi: 10.1016/j.ajog.2014.06.063. Am J Obstet Gynecol. 2014. PMID: 25168064 Free PMC article. No abstract available.
References
-
- Combs CA, Laros RK., Jr Prolonged third stage of labor: Morbidity and risk factors. Obstet Gynecol. Jun. 1991;77(6):863–7. - PubMed
-
- Dombrowski MP, Bottoms SF, Saleh AA, Hurd WW, Romero R. Third stage of labor: Analysis of duration and clinical practice. Am J Obstet Gynecol. 1995 Apr;172(4 Pt 1):1279–84. - PubMed
-
- Cheung WM, Hawkes A, Ibish S, Weeks AD. The retained placenta: Historical and geographical rate variations. J Obstet Gynaecol. 2011;31(1):37–42. - PubMed
-
- Prager SW, Oyer DJ. Second-trimester surgical abortion. Clin Obstet Gynecol. Jun. 2009;52(2):179–87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
