

The pathophysiology of hypertension in patients with obesity
- PMID: 24732974
- PMCID: PMC4308954
- DOI: 10.1038/nrendo.2014.44
The pathophysiology of hypertension in patients with obesity
Abstract
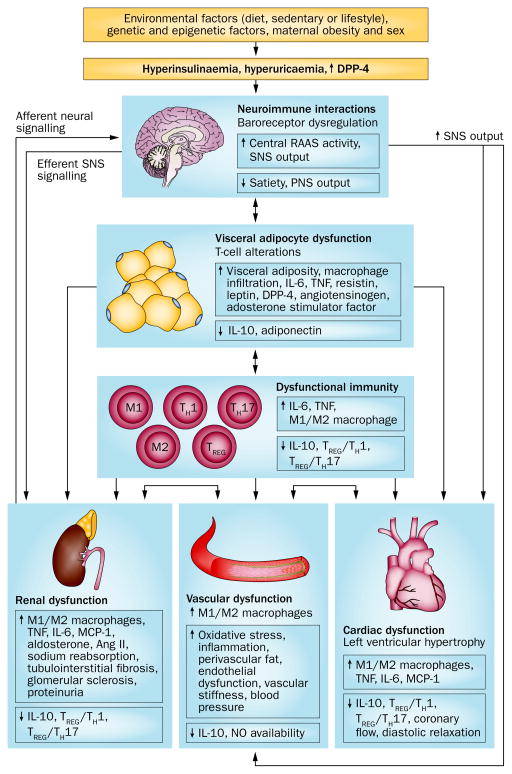
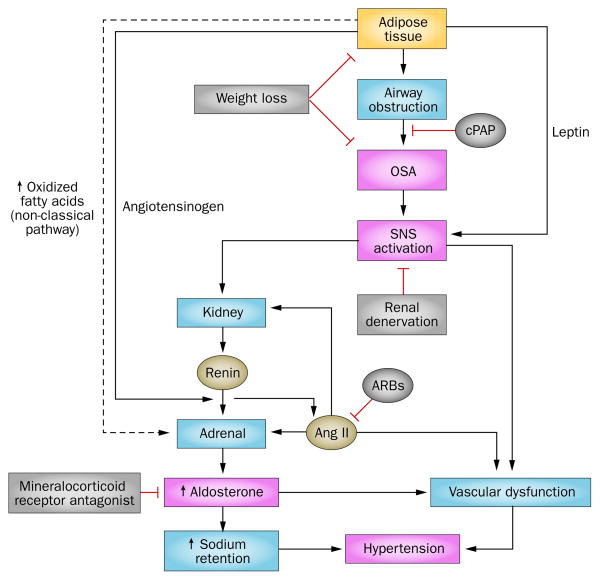
The combination of obesity and hypertension is associated with high morbidity and mortality because it leads to cardiovascular and kidney disease. Potential mechanisms linking obesity to hypertension include dietary factors, metabolic, endothelial and vascular dysfunction, neuroendocrine imbalances, sodium retention, glomerular hyperfiltration, proteinuria, and maladaptive immune and inflammatory responses. Visceral adipose tissue also becomes resistant to insulin and leptin and is the site of altered secretion of molecules and hormones such as adiponectin, leptin, resistin, TNF and IL-6, which exacerbate obesity-associated cardiovascular disease. Accumulating evidence also suggests that the gut microbiome is important for modulating these mechanisms. Uric acid and altered incretin or dipeptidyl peptidase 4 activity further contribute to the development of hypertension in obesity. The pathophysiology of obesity-related hypertension is especially relevant to premenopausal women with obesity and type 2 diabetes mellitus who are at high risk of developing arterial stiffness and endothelial dysfunction. In this Review we discuss the relationship between obesity and hypertension with special emphasis on potential mechanisms and therapeutic targeting that might be used in a clinical setting.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Hypertension in obesity: the role of hypothalamic inflammation.Nat Rev Endocrinol. 2014 Dec;10(12):760. doi: 10.1038/nrendo.2014.44-c1. Epub 2014 Oct 14. Nat Rev Endocrinol. 2014. PMID: 25311394 No abstract available.
References
-
- Malik VS, Willett WC, Hu FB. Global obesity: trends, risk factors and policy implications. Nat Rev Endocrinol. 2013;9:13–27. - PubMed
-
- Thomsen BL, Ekstrøm CT, Sørensen TI. Development of the obesity epidemic in Denmark: cohort, time and age effects among boys born 1930–1975. Int J Obes Relat Metab Disord. 1999;23:693–701. - PubMed
-
- Heimburger DC, et al. A festschrift for Roland L. Weinsier: nutrition scientist, educator, and clinician. Obes Res. 2003;11:1246–1262. - PubMed
-
- Keith SW, et al. Putative contributors to the secular increase in obesity: exploring the roads less traveled. Int J Obes (Lond) 2006;30:1585–1594. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
