

Effectiveness and safety of patient activation interventions for adults with type 2 diabetes: systematic review, meta-analysis, and meta-regression
- PMID: 24733301
- PMCID: PMC4099447
- DOI: 10.1007/s11606-014-2855-4
Effectiveness and safety of patient activation interventions for adults with type 2 diabetes: systematic review, meta-analysis, and meta-regression
Abstract
Background: Patient activation interventions (PAIs) engage patients in care by promoting increased knowledge, confidence, and/or skills for disease self-management. However, little is known about the impact of these interventions on a wide range of outcomes for adults with type 2 diabetes (DM2), or which of these interventions, if any, have the greatest impact on glycemic control.
Methods: Electronic databases were searched from inception through November 2011. Of 16,290 citations, two independent reviewers identified 138 randomized trials comparing PAIs to usual care/control groups in adults with DM2 that reported intermediate or long-term outcomes or harms. For meta-analyses of continuous outcomes, we used a random-effects model to derive pooled weighted mean differences (WMD). For all-cause mortality, we calculated the pooled odds ratio (OR) using Peto's method. We assessed statistical heterogeneity using the I (2) statistic and conducted meta-regression using a random-effects model when I (2) > 50 %. A priori meta-regression primary variables included: intervention strategies, intervention leader, baseline outcome value, quality, and study duration.
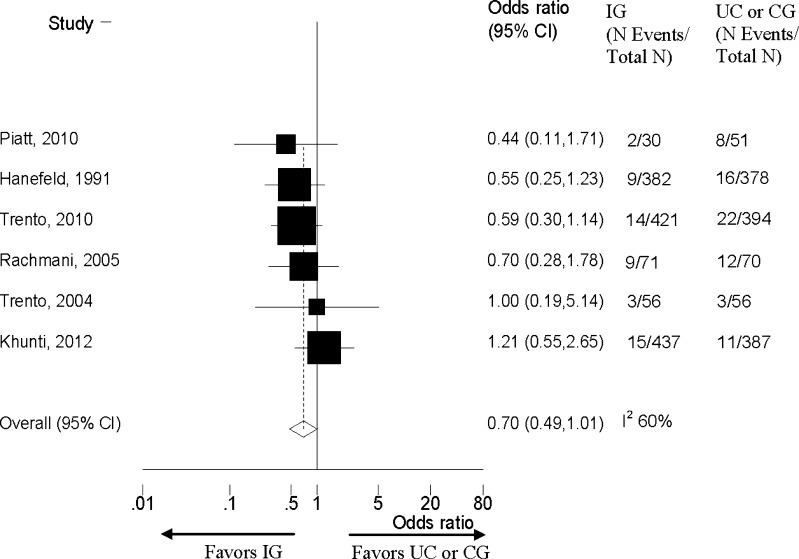
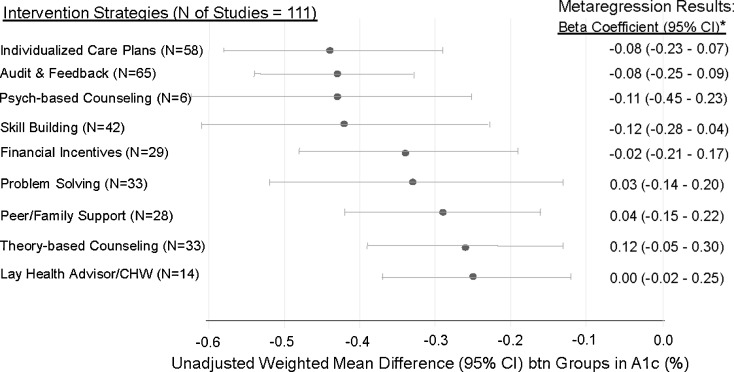
Results: PAIs modestly reduced intermediate outcomes [A1c: WMD 0.37 %, CI 0.28-0.45 %, I (2) 83 %; SBP: WMD 2.2 mmHg, CI 1.0-3.5 mmHg, I (2) 72 %; body weight: WMD 2.3 lbs, CI 1.3-3.2 lbs, I (2) 64 %; and LDL-c: WMD 4.2 mg/dL, CI 1.5-6.9 mg/dL, I (2) 64 %]. The evidence was moderate for A1c, low/very low for other intermediate outcomes, low for long-term mortality and very low for complications. Interventions had no effect on hypoglycemia (evidence: low) or short-term mortality (evidence: moderate). Higher baseline A1c, pharmacist-led interventions, and longer follow-up were associated with larger A1c improvements. No intervention strategy outperformed any other in adjusted meta-regression.
Conclusions: PAIs modestly improve A1c in adults with DM2 without increasing short-term mortality. These results support integration of these interventions into primary care for adults with uncontrolled glycemia, and provide evidence to insurers who do not yet cover these programs.
Figures
Similar articles
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Unconditional cash transfers for reducing poverty and vulnerabilities: effect on use of health services and health outcomes in low- and middle-income countries.Cochrane Database Syst Rev. 2022 Mar 29;3(3):CD011135. doi: 10.1002/14651858.CD011135.pub3. Cochrane Database Syst Rev. 2022. PMID: 35348196 Free PMC article.
Cited by
-
Talking the same language on patient empowerment: Development and content validation of a taxonomy of self-management interventions for chronic conditions.Health Expect. 2021 Oct;24(5):1626-1638. doi: 10.1111/hex.13303. Epub 2021 Jul 12. Health Expect. 2021. PMID: 34252259 Free PMC article.
-
Self-regulation mechanisms in health behavior change: a systematic meta-review of meta-analyses, 2006-2017.Health Psychol Rev. 2020 Mar;14(1):6-42. doi: 10.1080/17437199.2019.1679654. Health Psychol Rev. 2020. PMID: 31662031 Free PMC article.
-
A Patient-Facing Diabetes Dashboard Embedded in a Patient Web Portal: Design Sprint and Usability Testing.JMIR Hum Factors. 2018 Sep 24;5(3):e26. doi: 10.2196/humanfactors.9569. JMIR Hum Factors. 2018. PMID: 30249579 Free PMC article.
-
Social determinants of health in adults with type 2 diabetes--Contribution of mutable and immutable factors.Diabetes Res Clin Pract. 2015 Nov;110(2):193-201. doi: 10.1016/j.diabres.2015.09.007. Epub 2015 Sep 18. Diabetes Res Clin Pract. 2015. PMID: 26411692 Free PMC article.
-
Association between patient activation, self-management behaviours and clinical outcomes in adults with type 2 diabetes: a systematic review with narrative synthesis.BMJ Open. 2025 May 27;15(5):e095456. doi: 10.1136/bmjopen-2024-095456. BMJ Open. 2025. PMID: 40436451 Free PMC article.
References
-
- National Diabetes Fact Sheet, 2011. Available at http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2011.pdf. 2011. Accessed 3-5-2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
