

Screening, assessment, and care of anxiety and depressive symptoms in adults with cancer: an American Society of Clinical Oncology guideline adaptation
- PMID: 24733793
- PMCID: PMC4090422
- DOI: 10.1200/JCO.2013.52.4611
Screening, assessment, and care of anxiety and depressive symptoms in adults with cancer: an American Society of Clinical Oncology guideline adaptation
Abstract
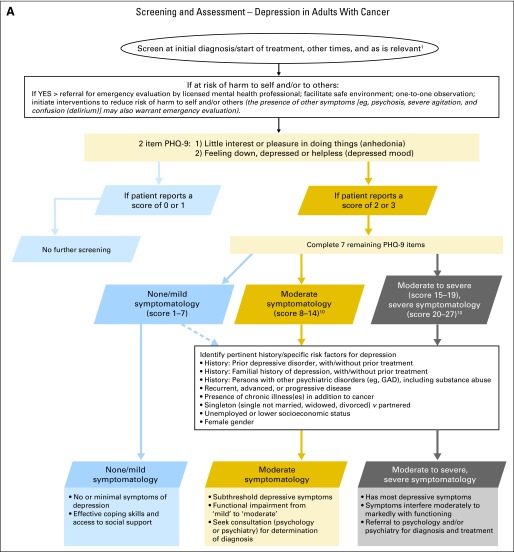
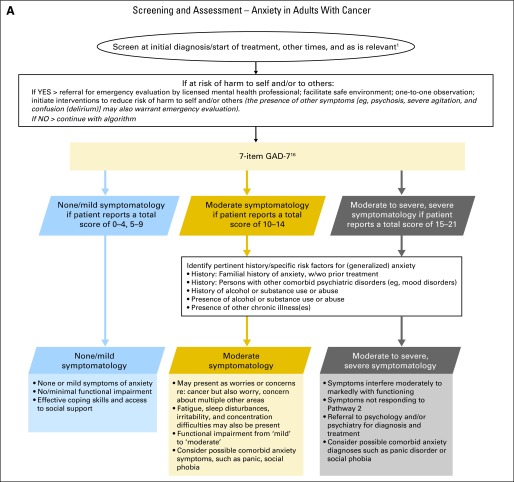
Purpose: A Pan-Canadian Practice Guideline on Screening, Assessment, and Care of Psychosocial Distress (Depression, Anxiety) in Adults With Cancer was identified for adaptation.
Methods: American Society of Clinical Oncology (ASCO) has a policy and set of procedures for adapting clinical practice guidelines developed by other organizations. The guideline was reviewed for developmental rigor and content applicability.
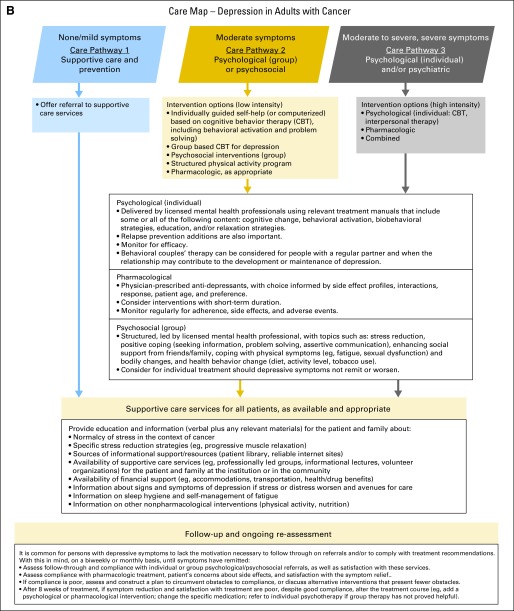
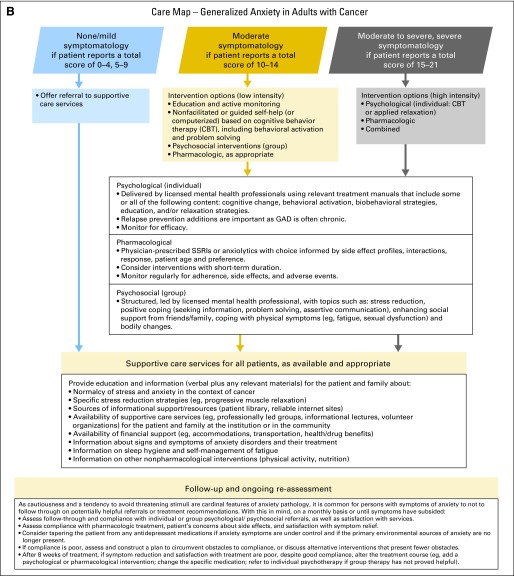
Results: On the basis of content review of the pan-Canadian guideline, the ASCO panel agreed that, in general, the recommendations were clear, thorough, based on the most relevant scientific evidence, and presented options that will be acceptable to patients. However, for some topics addressed in the pan-Canadian guideline, the ASCO panel formulated a set of adapted recommendations based on local context and practice beliefs of the ad hoc panel members. It is recommended that all patients with cancer be evaluated for symptoms of depression and anxiety at periodic times across the trajectory of care. Assessment should be performed using validated, published measures and procedures. Depending on levels of symptoms and supplementary information, differing treatment pathways are recommended. Failure to identify and treat anxiety and depression increases the risk for poor quality of life and potential disease-related morbidity and mortality. This guideline adaptation is part of a larger survivorship guideline series.
Conclusion: Although clinicians may not be able to prevent some of the chronic or late medical effects of cancer, they have a vital role in mitigating the negative emotional and behavioral sequelae. Recognizing and treating effectively those who manifest symptoms of anxiety or depression will reduce the human cost of cancer.
© 2014 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Howell D, Keller-Olaman S, Oliver T, et al. A pan-Canadian practice guideline: Screening, assessment and care of psychosocial distress (depression, anxiety) in adults with cancer. Canadian Partnership Against Cancer (Cancer Journey Action Group) and the Canadian Association of Psychosocial Oncology, 2010. www.capo.ca/pdf/ENGLISH_Depression_Anxiety_Guidelines_for_Posting_Sept20....
-
- American Cancer Society. Cancer treatment and survivorship facts & figures 2012-2013. American Cancer Society, 2012. www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/doc....
-
- Hewitt M, Greenfield S, Stovall EE. Washington, DC: The National Academies Press; 2006. From Cancer Patient to Cancer Survivor: Lost in Transition.
-
- Ganz PA, Earle CC, Goodwin PJ. Journal of Clinical Oncology update on progress in cancer survivorship care and research. J Clin Oncol. 2012;30:3655–3656. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
