

Sleep apnea and 20-year follow-up for all-cause mortality, stroke, and cancer incidence and mortality in the Busselton Health Study cohort
- PMID: 24733978
- PMCID: PMC3960375
- DOI: 10.5664/jcsm.3600
Sleep apnea and 20-year follow-up for all-cause mortality, stroke, and cancer incidence and mortality in the Busselton Health Study cohort
Abstract
Objective: To ascertain whether objectively measured obstructive sleep apnea (OSA) independently increases the risk of all cause death, cardiovascular disease (CVD), coronary heart disease (CHD), stroke or cancer.
Design: Community-based cohort.
Setting and participants: 400 residents of the Western Australian town of Busselton.
Measures: OSA severity was quantified via the respiratory disturbance index (RDI) as measured by a single night recording in November-December 1990 using the MESAM IV device, along with a range of other risk factors. Follow-up for deaths and hospitalizations was ascertained via record linkage to the end of 2010.
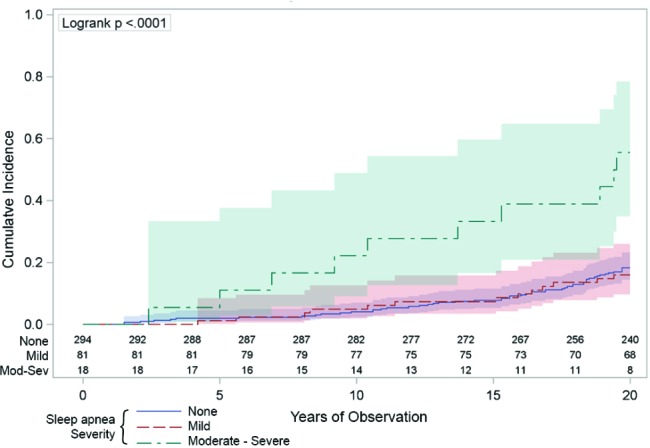
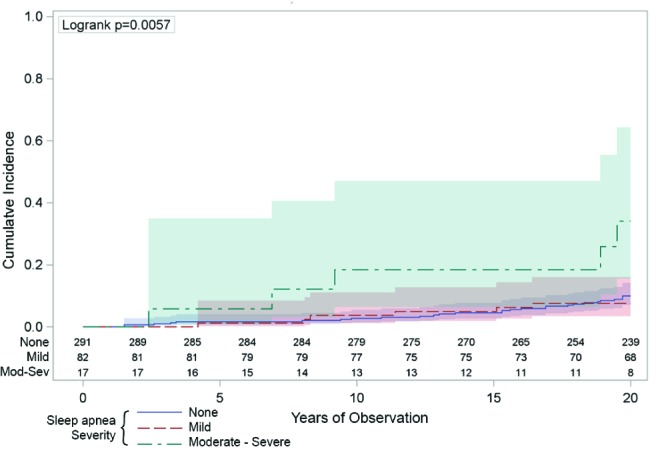
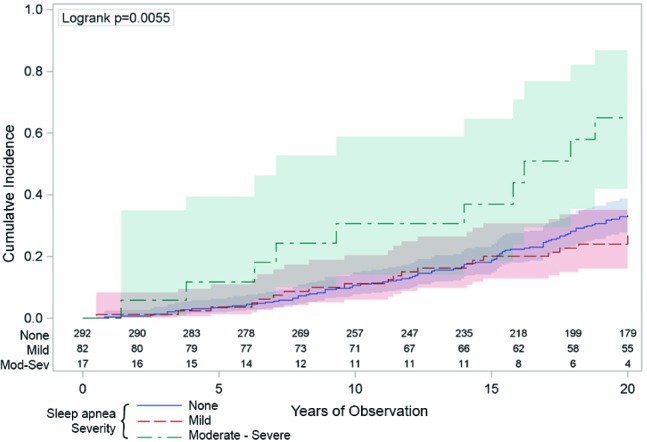
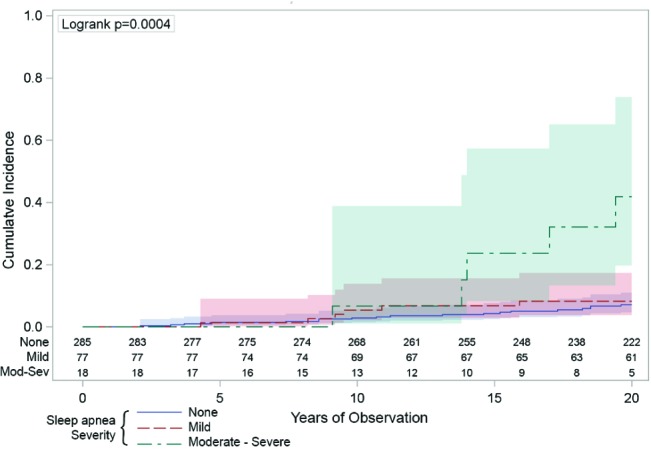
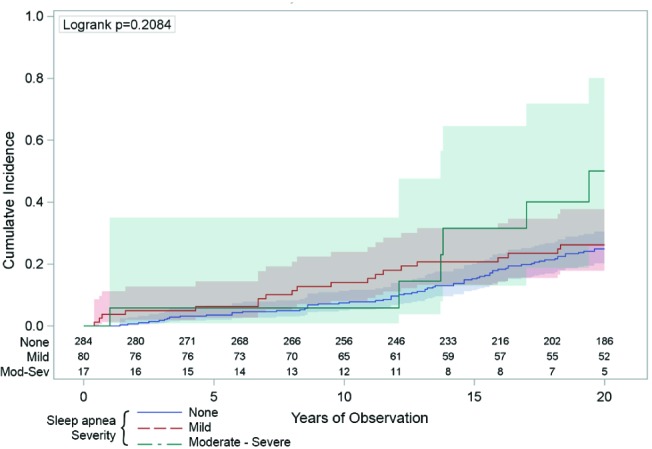
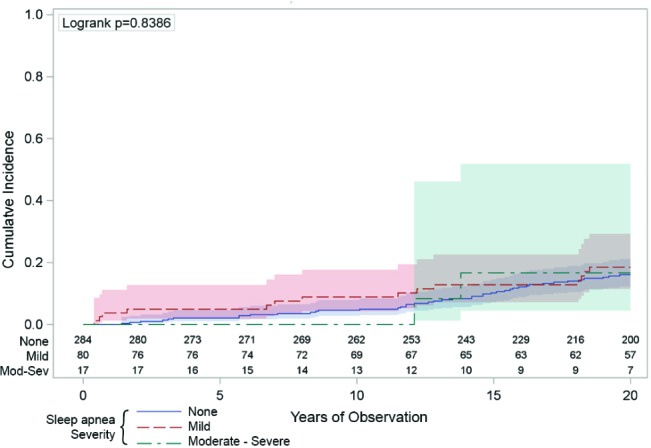
Results: We had follow-up data in 397 people and then removed those with a previous stroke (n = 4) from the mortality/ CVD/CHD/stroke analyses and those with cancer history from the cancer analyses (n = 7). There were 77 deaths, 103 cardiovascular events (31 strokes, 59 CHD) and 125 incident cases of cancer (39 cancer fatalities) during 20 years follow-up. In fully adjusted models, moderate-severe OSA was significantly associated with all-cause mortality (HR = 4.2; 95% CI 1.9, 9.2), cancer mortality (3.4; 1.1, 10.2), incident cancer (2.5; 1.2, 5.0), and stroke (3.7; 1.2, 11.8), but not significantly with CVD (1.9; 0.75, 4.6) or CHD incidence (1.1; 0.24, 4.6). Mild sleep apnea was associated with a halving in mortality (0.5; 0.27, 0.99), but no other outcome, after control for leading risk factors.
Conclusions: Moderate-to-severe sleep apnea is independently associated with a large increased risk of all-cause mortality, incident stroke, and cancer incidence and mortality in this community-based sample.
Keywords: Sleep disordered breathing; coronary artery disease; melanoma.
Figures
Comment in
-
Emerging from the shadows: a possible link between sleep apnea and cancer.J Clin Sleep Med. 2014 Apr 15;10(4):363-4. doi: 10.5664/jcsm.3602. J Clin Sleep Med. 2014. PMID: 24733979 Free PMC article. No abstract available.
-
Sleep apnea 20/20: a 20-year cohort that continues to inform the next 20 years.J Clin Sleep Med. 2020 Dec 17;16(S1):27-28. doi: 10.5664/jcsm.8894. J Clin Sleep Med. 2020. PMID: 33054968 Free PMC article.
References
-
- Munoz R, Duran-Cantolla J, Martinez-Vila E, et al. Severe sleep apnea and risk of ischemic stroke in the elderly. Stroke. 2006;37:2317–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
