

Feasibility of endoscopic treatment of middle ear myoclonus: a cadaveric study
- PMID: 24734199
- PMCID: PMC3964766
- DOI: 10.1155/2014/175268
Feasibility of endoscopic treatment of middle ear myoclonus: a cadaveric study
Abstract
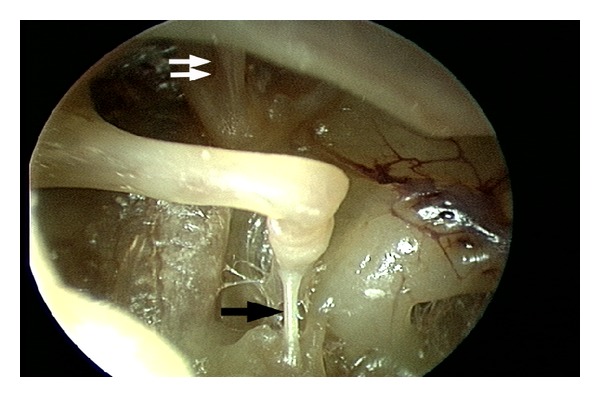
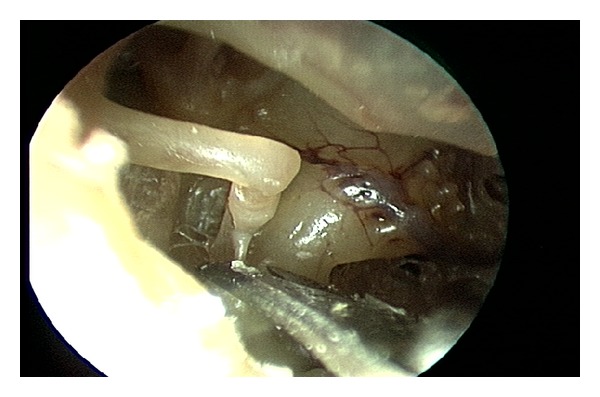
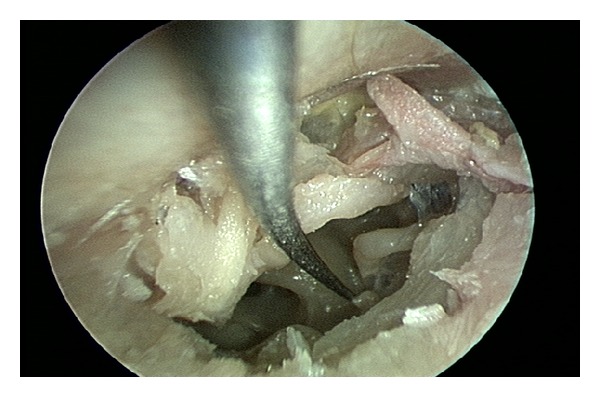
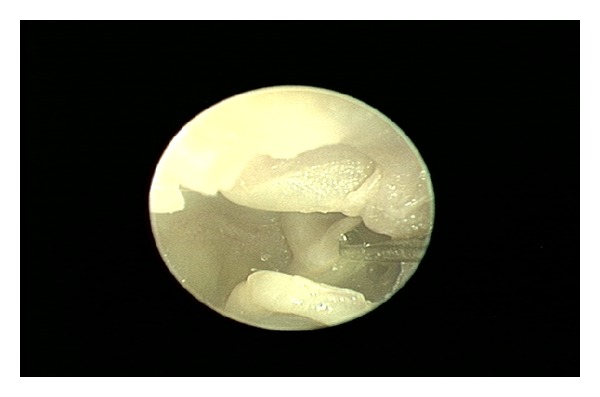
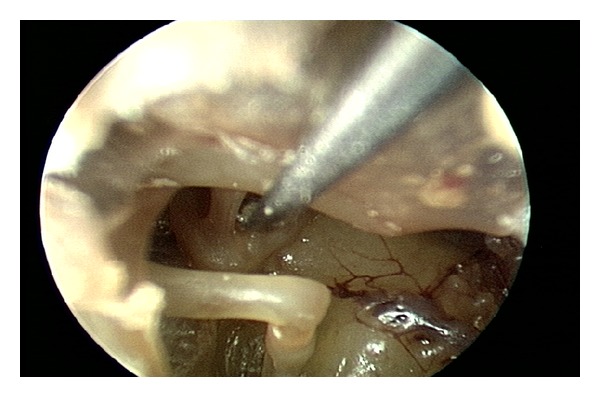
Stapedius and tensor tympani tenotomy is a relatively simple surgical procedure commonly performed to control pulsatile tinnitus due to middle ear myoclonus and for several other indications. We designed a cadaveric study to assess the feasibility of an entirely endoscopic approach to stapedius and tensor tympani tenotomy. We performed this endoscopic ear surgery in 10 cadaveric temporal bones and summarized our experience. Endoscopic stapedius and tensor tympani section is a new, minimally invasive treatment option for middle ear myoclonus that should be considered as the first line surgical approach in patients who fail medical therapy. The use of an endoscopic approach allows for easier access and vastly superior visualization of the relevant anatomy, which in turn allows the surgeon to minimize tissue dissection. The entire operation, including raising the tympanomeatal flap and tendon section, can be safely completed under visualization with a rigid endoscope.
Figures

Similar articles
-
Middle ear myoclonus cured by selective tenotomy of the tensor tympani: strategies for targeted intervention for middle ear muscles.Otol Neurotol. 2013 Dec;34(9):1552-8. doi: 10.1097/MAO.0000000000000126. Otol Neurotol. 2013. PMID: 24232057
-
Transcanal Endoscopic Stapedial and Tensor Tympani Tenotomy for Middle Ear Myoclonus: A Retrospective Case Series of Surgical Outcomes.Otol Neurotol. 2023 Jun 1;44(5):478-482. doi: 10.1097/MAO.0000000000003863. Epub 2023 Mar 24. Otol Neurotol. 2023. PMID: 37026830
-
Middle ear myoclonus: Systematic review of results and complications for various treatment approaches.Am J Otolaryngol. 2022 Jan-Feb;43(1):103228. doi: 10.1016/j.amjoto.2021.103228. Epub 2021 Sep 15. Am J Otolaryngol. 2022. PMID: 34537509
-
[Effect of the stapedius and tensor tympani muscles tenotomy on the quality of life of patients suffering from Ménière's disease].Orv Hetil. 2020 Feb;161(5):177-182. doi: 10.1556/650.2020.31634. Orv Hetil. 2020. PMID: 31984774 Hungarian.
-
[Diagnosis and treatment of middle ear myoclonic tinnitus].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2024 Nov;38(11):1081-1084. doi: 10.13201/j.issn.2096-7993.2024.11.017. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2024. PMID: 39534904 Free PMC article. Review. Chinese.
Cited by
-
Transcanal endoscopic myringoplasty: a case series in a university center.Braz J Otorhinolaryngol. 2016 May-Jun;82(3):321-5. doi: 10.1016/j.bjorl.2015.05.012. Epub 2015 Nov 6. Braz J Otorhinolaryngol. 2016. PMID: 26642752 Free PMC article.
-
Pain After Ear Surgery: A Prospective Evaluation of Endoscopic and Microscopic Approaches.Laryngoscope. 2021 May;131(5):1127-1131. doi: 10.1002/lary.29038. Epub 2020 Sep 18. Laryngoscope. 2021. PMID: 32945553 Free PMC article.
-
COVID-19-Associated Middle Ear Myoclonus in a 10-Year-Old Male.Cureus. 2022 Apr 28;14(4):e24550. doi: 10.7759/cureus.24550. eCollection 2022 Apr. Cureus. 2022. PMID: 35651465 Free PMC article.
-
Endoscopic and minimally-invasive ear surgery: A path to better outcomes.World J Otorhinolaryngol Head Neck Surg. 2017 Sep 22;3(3):129-135. doi: 10.1016/j.wjorl.2017.08.001. eCollection 2017 Sep. World J Otorhinolaryngol Head Neck Surg. 2017. PMID: 29516056 Free PMC article.
References
-
- Bhimrao SK, Masterson L, Baguley D. Systematic review of management strategies for middle ear myoclonus. Otolaryngology. 2012;146:698–706. - PubMed
-
- Hidaka H, Honkura Y, Ota J, et al. Middle ear myoclonus cured by selective tenotomy of the tensor tympani: strategies for targeted intervention for middle ear muscles. Otology and Neurotology. 2013;34:1552–1558. - PubMed
-
- Zipfel TE, Kaza SR, Greene JS. Middle-ear myoclonus. Journal of Laryngology and Otology. 2000;114(3):207–209. - PubMed
-
- Park SN, Bae SC, Lee GH, et al. Clinical characteristics and therapeutic response of objective tinnitus due to middle ear myoclonus: a large case series. Laryngoscope. 2013;123:2516–2520. - PubMed
-
- Badia L, Parikh A, Brookes GB. Management of middle ear myoclonus. Journal of Laryngology and Otology. 1994;108(5):380–382. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
