

Multimodality imaging features, metastatic pattern and clinical outcome in adult extraskeletal Ewing sarcoma: experience in 26 patients
- PMID: 24734938
- PMCID: PMC4075565
- DOI: 10.1259/bjr.20140123
Multimodality imaging features, metastatic pattern and clinical outcome in adult extraskeletal Ewing sarcoma: experience in 26 patients
Abstract
Objective: To describe the multimodality imaging features, metastatic pattern and clinical outcome in adult extraskeletal Ewing sarcoma (EES).
Methods: In this institutional review board-approved, health insurance portability and accountability act-compliant retrospective study, we included 26 patients (17 females and 9 males; mean age, 36 years; range, 18-85 years) with pathologically confirmed EES seen at our institute between 1999 and 2011, who had imaging of primary tumour. Imaging of primary tumour in all 26 patients and follow-up imaging in 23 was reviewed by two radiologists in consensus. Clinical data were extracted from electronic medical records.
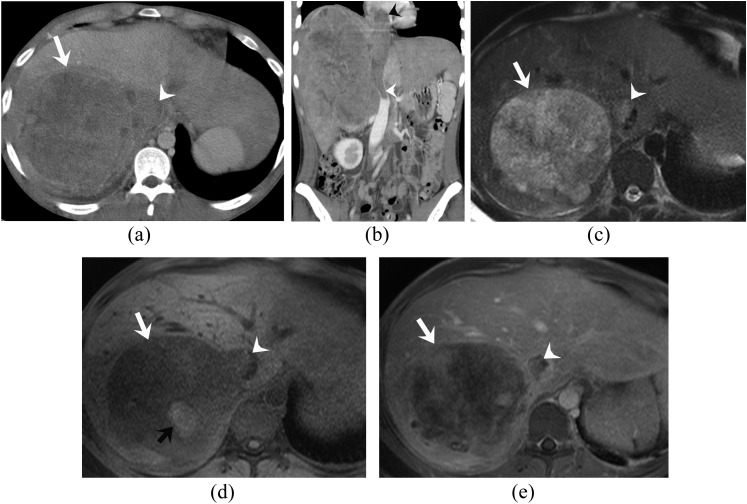
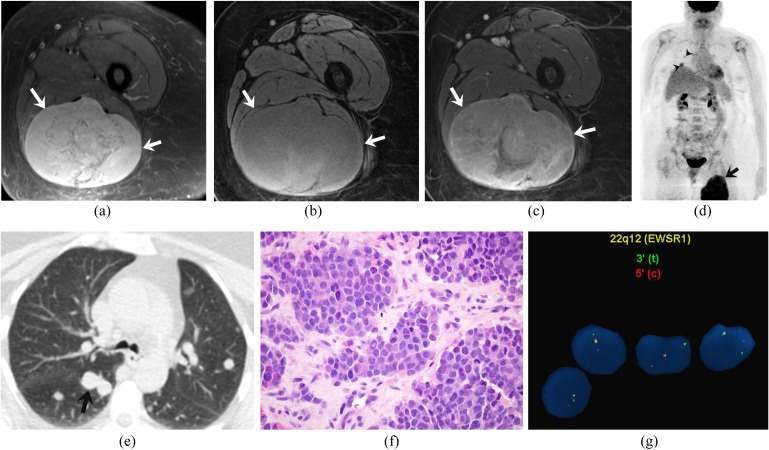
Results: The most common primary sites were the torso (n = 13), extremities (n = 10) and head and neck (HN) region (n = 3). The mean tumour size was 9 cm (range, 3-22 cm); tumours of the torso were larger than those of other areas (p > 0.05). Compared with the skeletal muscle, tumours were isodense on CT (21/21), hypointense (n = 5) to isointense (n = 14) on T1 weighted image, hyperintense on T2 weighted image (19/19) and were fluorine-18 fludeoxyglucose ((18)F-FDG)-avid [10/10; mean maximum standardized uptake value of 7 (range, 3-11)]. Necrosis (15/26), haemorrhage (5/26) and adjacent organ invasion (14/26) were present without calcification. Median follow-up was 16 months. 5 patients had local recurrence (torso, 3; extremity, 1; and HN, 1). Metastases developed in 11 patients (torso, 7; extremities, 3; and HN, 1; p > 0.05); 8 at presentation, most commonly to lung (9/11), peritoneum (4/11), muscles (4/11) and lymph nodes (4/11). Nine patients (torso, 7; extremity, 1; and HN, 1) died (10 months median survival) (p > 0.05).
Conclusion: Adult EESs are large tumours, which frequently invade adjacent organs and metastasize to the lung. EESs of the torso are larger, have more frequent metastases and poorer outcomes.
Advances in knowledge: Adult EESs of the torso have poor outcomes compared with other EESs.
Figures
References
-
- Quesada J, Amato R. The molecular biology of soft-tissue sarcomas and current trends in therapy. Sarcoma 2012; 2012: 849456. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22665999. doi: 10.1155/2012/849456 - DOI - PMC - PubMed
-
- Murphey MD, Senchak LT, Mambalam PK, Logie CI, Klassen-Fischer MK, Kransdorf MJ. From the radiologic pathology archives: ewing sarcoma family of tumors: radiologic-pathologic correlation. Radiographics 2013; 33: 803–31. - PubMed
-
- Jawad MU, Cheung MC, Min ES, Schneiderbauer MM, Koniaris LG, Scully SP. Ewing sarcoma demonstrates racial disparities in incidence-related and sex-related differences in outcome: an analysis of 1631 cases from the SEER database, 1973-2005. Cancer 2009; 115: 3526–36. doi: 10.1002/cncr.24388 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
