

Can comprehensive specialised end-of-life care be provided at home? Lessons from a study of an innovative consultant-led community service in the UK
- PMID: 24735122
- PMCID: PMC4359037
- DOI: 10.1111/ecc.12195
Can comprehensive specialised end-of-life care be provided at home? Lessons from a study of an innovative consultant-led community service in the UK
Abstract
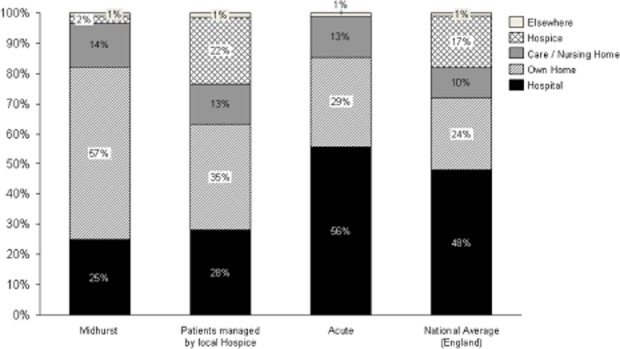
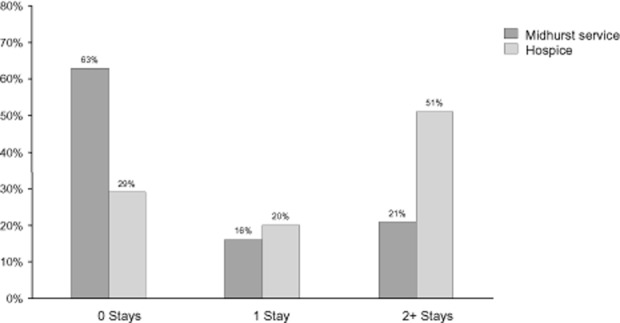
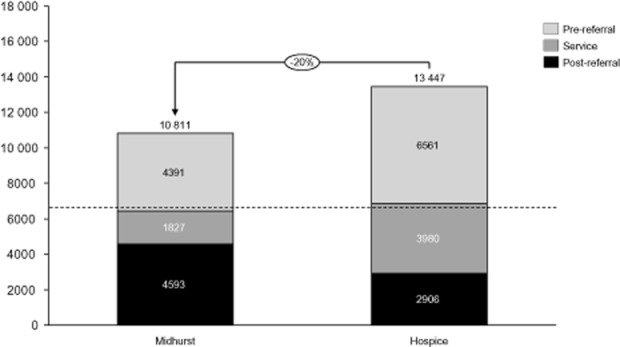
The Midhurst Macmillan Specialist Palliative Care Service (MMSPCS) is a UK, medical consultant-led, multidisciplinary team aiming to provide round-the-clock advice and care, including specialist interventions, in the home, community hospitals and care homes. Of 389 referrals in 2010/11, about 85% were for cancer, from a population of about 155 000. Using a mixed method approach, the evaluation comprised: a retrospective analysis of secondary-care use in the last year of life; financial evaluation of the MMSPCS using an Activity Based Costing approach; qualitative interviews with patients, carers, health and social care staff and MMSPCS staff and volunteers; a postal survey of General Practices; and a postal survey of bereaved caregivers using the MMSPCS. The mean cost is about 3000 GBP (3461 EUR) per patient with mean cost of interventions for cancer patients in the last year of life 1900 GBP (2192 EUR). Post-referral, overall costs to the system are similar for MMSPCS and hospice-led models; however, earlier referral avoided around 20% of total costs in the last year of life. Patients and carers reported positive experiences of support, linked to the flexible way the service worked. Seventy-one per cent of patients died at home. This model may have application elsewhere.
Keywords: end-of-life care; home care services; home death; mixed methods evaluation.; preferred place of care/death; specialist palliative care.
© 2014 The Authors. European Journal of Cancer Care published by John Wiley & Sons Ltd.
Figures
References
-
- Beck-Friis B. Strang P. The organization of hospital-based home care for terminally ill cancer patients: the Motala model. Palliative Medicine. 1993;7:93–100. - PubMed
-
- Brazil K, Howell D, Bedard M, Krueger P. Heidbrecht C. Preferences for place of care and place of death among informal caregivers of the terminally ill. Palliative Medicine. 2005;9:492–499. - PubMed
-
- Brazil K, Kassalainen S, Ploeg J. Marshall D. Moral distress experienced by health care professionals who provide home-based palliative care. Social Science and Medicine (1982) 2010;71:1687–1691. - PubMed
-
- Brown L. Walter T. Towards a social model of end-of-life care. British Journal of Social Work. 2013 & doi: . - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
