

Fixed-dose combination therapy for the prevention of cardiovascular disease
- PMID: 24737108
- PMCID: PMC4083498
- DOI: 10.1002/14651858.CD009868.pub2
Fixed-dose combination therapy for the prevention of cardiovascular disease
Update in
-
Fixed-dose combination therapy for the prevention of atherosclerotic cardiovascular diseases.Cochrane Database Syst Rev. 2017 Mar 6;3(3):CD009868. doi: 10.1002/14651858.CD009868.pub3. Cochrane Database Syst Rev. 2017. PMID: 28263370 Free PMC article.
Abstract
Background: Cardiovascular disease (CVD) is the leading cause of death and disability worldwide, yet CVD risk factor control and secondary prevention rates remain low. A fixed-dose combination of blood pressure and cholesterol lowering and antiplatelet treatments into a single pill, or polypill, has been proposed as one strategy to reduce the global burden of CVD by up to 80% given its potential for better adherence and lower costs.
Objectives: To determine the effectiveness of fixed-dose combination therapy on reducing fatal and non-fatal CVD events and on improving blood pressure and lipid CVD risk factors for both primary and secondary prevention of CVD. We also aimed to determine discontinuation rates, adverse events, health-related quality of life, and costs of fixed-dose combination therapy.
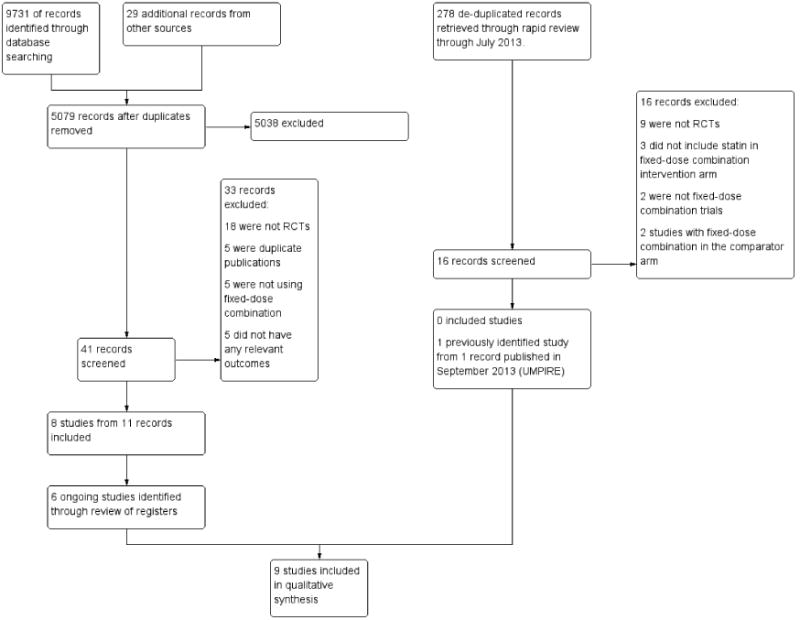
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library (2013, Issue 6), MEDLINE Ovid (1946 to week 2 July 2013), EMBASE Ovid (1980 to Week 28 2013), ISI Web of Science (1970 to 19 July 2013), and the Database of Abstracts of Reviews of Effects (DARE), Health Technology Assessment Database (HTA), and Health Economics Evaluations Database (HEED) (2011, Issue 4) in The Cochrane Library. We used no language restrictions.
Selection criteria: We included randomised controlled trials of a fixed-dose combination therapy including at least one blood pressure lowering and one lipid lowering component versus usual care, placebo, or a single drug active component for any treatment duration in adults ≥ 18 years old with no restrictions on presence or absence of pre-existing cardiovascular disease.
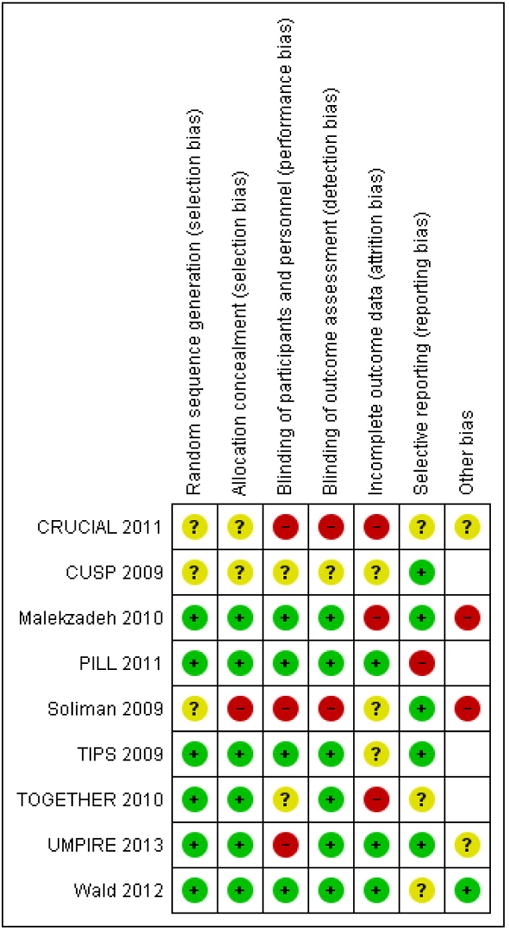
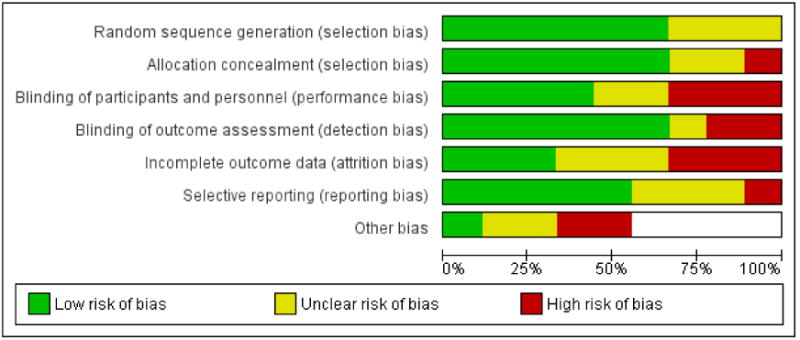
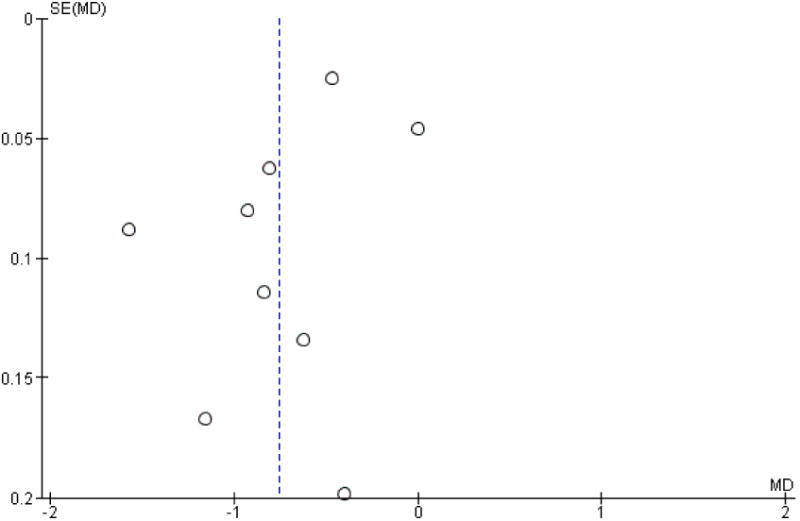
Data collection and analysis: Three review authors independently selected studies for inclusion and extracted the data. We evaluated risk of bias using the Cochrane risk of bias assessment tool. We sought to include outcome data on all-cause mortality, fatal and non-fatal CVD events, adverse events, changes in systolic and diastolic blood pressure, total and low density lipoprotein (LDL) cholesterol concentrations, discontinuation rates, quality of life, and costs. We calculated risk ratios (RR) for dichotomous data and weighted mean differences (MD) for continuous data with 95% confidence intervals (CI) using fixed-effect models when heterogeneity was low (I(2) < 50%) and random-effects models when heterogeneity was high (I(2) > 50%).
Main results: We found nine randomised controlled trials with a total of 7047 participants. Seven of the nine trials evaluated the effects of fixed-dose combination therapy on primary CVD prevention, and the trial length ranged from six weeks to 15 months. We found a moderate to high risk of bias in the domains of selection, performance, detection, attrition, and other types of bias in five of the nine trials. Compared with the comparator groups, the effects of the fixed-dose combination treatment on mortality (1.2% versus 1.0%, RR 1.26, 95% CI 0.67 to 2.38, N = 3465) and cardiovascular events (4.0% versus 2.9%, RR 1.38, 95% CI 0.91 to 2.10, N = 2479) were uncertain (low quality evidence). The low event rates for these outcomes, limited availability of data as only two out of nine trials reported on these outcomes, and a high risk of bias in at least one domain suggest that these results should not be viewed with confidence. Adverse events were common in both the intervention (30%) and comparator (24%) groups, with participants randomised to fixed-dose combination therapy being 20% (95% CI 9% to 30%) more likely to report an adverse event. Notably, no serious adverse events were reported. Compared with placebo, the rate of discontinuation among participants randomised to fixed-dose combination was higher (14% versus 11%, RR 1.26 95% CI 1.02 to 1.55). The weighted mean differences in systolic and diastolic blood pressure between the intervention and control arms were -7.05 mmHg (95% CI -10.18 to -3.87) and -3.65 mmHg (95% CI -5.44 to -1.85), respectively. The weighted mean differences (95% CI) in total and LDL cholesterol between the intervention and control arms were -0.75 mmol/L (95% CI -1.05 to -0.46) and -0.81 mmol/L (95% CI -1.09 to -0.53), respectively. There was a high degree of statistical heterogeneity in comparisons of blood pressure and lipids (I(2) ≥ 70% for all) that could not be explained, so these results should be viewed with caution. Fixed-dose combination therapy improved adherence to a multi-drug strategy by 33% (26% to 41%) compared with usual care, but this comparison was reported in only one study. The effects of fixed-dose combination therapy on quality of life are uncertain, though these results were reported in only one trial. No trials reported costs.
Authors' conclusions: Compared with placebo, single drug active component, or usual care, the effects of fixed-dose combination therapy on all-cause mortality or CVD events are uncertain; only few trials report these outcomes and the included trials were primarily designed to observe changes in CVD risk factor levels rather than clinical events. Reductions in blood pressure and lipid parameters are generally lower than those previously projected, though substantial heterogeneity of results exists. Fixed-dose combination therapy is associated with modest increases in adverse events compared with placebo, single drug active component, or usual care but may be associated with improved adherence to a multidrug regimen. Ongoing trials of fixed-dose combination therapy will likely inform key outcomes.
Figures
Update of
-
Fixed-dose combination therapy for the prevention of cardiovascular disease.Cochrane Database Syst Rev. 2012;(5):CD009868. doi: 10.1002/14651858.CD009868. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2014 Apr 16;(4):CD009868. doi: 10.1002/14651858.CD009868.pub2. PMID: 25267903 Free PMC article. Updated.
Comment in
-
Impact of polypill difficult to demonstrate from varied studies, say Cochrane reviewers.BMJ. 2014 Apr 16;348:g2819. doi: 10.1136/bmj.g2819. BMJ. 2014. PMID: 24742603 No abstract available.
-
One pill, four questions: what we still need to know about reducing cardiovascular risk with combination therapy.Cochrane Database Syst Rev. 2014 Apr 16;2014(4):ED000079. doi: 10.1002/14651858.ED000079. Cochrane Database Syst Rev. 2014. PMID: 24818243 Free PMC article. No abstract available.
-
Fixed-dose combination therapy (polypill) for the prevention of cardiovascular disease.JAMA. 2014 Nov 19;312(19):2030-1. doi: 10.1001/jama.2014.13616. JAMA. 2014. PMID: 25399279
References
References to studies included in this review
-
- Pavia LA, Erdine S, Zamorano J, Kim JH, Al KA, Westergaard M, et al. Cardiovascular risk factor management: Single-pill amlodipine/atorvastatin versus usual care in patients with hypertension and additional risk factors - the CRUCIAL trial. Journal of Hypertension. 2010:e278–9. Conference(various pagings)
-
- Pavia LA, Zamorano J, Kim JH, Erdine S, Al KA, Westergaard M, et al. Treatment strategies for cardiovascular risk factor management in patients with hypertension and additional risk factors-experiences from the usual care arm of the CRUCIAL trial. Journal of Hypertension. 2010:e276–7. Conference(various pagings)
-
- Zamorano J, Erdine S, Pavia A, Kim JH, Al-Khadra A, Westergaard M, et al. Proactive multiple cardiovascular risk factor management compared with usual care in patients with hypertension and additional risk factors: The CRUCIAL trial. Current Medical Research and Opinion. 2011;27(4):821–33. - PubMed
-
- Neutel JM, Bestermann WH, Dyess EM, Graff A, Kursun A, Sutradhar S, et al. The use of a single-pill calcium channel blocker/statin combination in the management of hypertension and dyslipidemia: A randomized, placebo-controlled, multicenter study. Journal of Clinical Hypertension. 2009;11(1):22–30. - PMC - PubMed
-
- Malekzadeh F, Marshall T, Pourshams A, Gharravi M, Aslani A, Nateghi A, et al. A pilot double-blind randomised placebo-controlled trial of the effects of fixed-dose combination therapy (‘polypill’) on cardiovascular risk factors. International Journal of Clinical Practice. 2010;64(9):1220–7. - PubMed
References to studies excluded from this review
-
- Avenell A, Maclennan GS, Jenkinson DJ, McPherson GC, McDonald AM, Pant PR, et al. Long-term follow-up for mortality and cancer in a randomized, placebo-controlled trial of vitamin D3 and/or calcium (RECORD) Journal of Clinical Endocrinology and Metabolism. 2012;97:614–22. - PubMed
-
- Bakris GL, Sica D, White WB, Cushman WC, Weber MA, Handley A, et al. Antihypertensive efficacy of hydrochlorothiazide vs chlorthalidone combined with azilsartan medoxomil. American Journal of Medicine. 2012;125:1229e1–10. - PubMed
-
- Ferdinand KC, Flack JM, Saunders E, Victor R, Watson K, Kursun A, et al. Amlodipine/atorvastatin single-pill therapy for blood pressure and lipid goals in African Americans: influence of the metabolic syndrome and type 2 diabetes mellitus. Journal of Clinical Hypertension. 2009;11(10):585–93. - PMC - PubMed
References to ongoing studies
-
- Sanz G, Fuster V, Guzmán L, Guglietta A, Arnáiz JA, Martínez F, et al. The fixed-dose combination drug for secondary cardiovascular prevention project: study design and objectives. American Heart Journal. 2011;162:811–7. - PubMed
-
- Selak V, Elley CR, Crengle S, Harwood M, Doughty R, Arroll B, et al. Improving adherence using combination therapy (IMPACT): design and protocol of a RCT in primary care. Contemporary Clinical Trials. 2011;32:909–15. - PubMed
-
- Liu H, Patel A, Brown A, Eades S, Hayman N, Jan S, et al. Rationale and design of the Kanyini guidelines adherence with the polypill (Kanyini-GAP) study: a randomised controlled trial of a polypill-based strategy amongst indigenous and non indigenous people at high cardiovascular risk. BMC Public Health. 2010;10:458. - PMC - PubMed
-
-
Polypill and non-alcoholic steatohepatitis (PolyIran-L).
Clinicaltrials.gov : NCT01245608.
-
-
-
Prevention of cardiovascular disease in middle-aged and elderly Iranians using a single polypill (PolyIran).
Clinicaltrials.gov : NCT01271985.
-
Additional references
-
- ALLHAT-investigators. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) JAMA. 2002;288(23):2981–97. - PubMed
-
- Armitage JM, Bowman L, Clarke RJ, Wallendszus K, Bulbulia R, Rahimi K, et al. Effects of homocysteine-lowering with folic acid plus vitamin B12 vs placebo on mortality and major morbidity in myocardial infarction survivors: a randomized trial. JAMA. 2010;303(24):2486–94. - PubMed
-
- Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366(9493):1267–78. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical