

Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: the foundation for the National Institutes of Health (FNIH) sarcopenia project
- PMID: 24737560
- PMCID: PMC3991140
- DOI: 10.1093/gerona/glu012
Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: the foundation for the National Institutes of Health (FNIH) sarcopenia project
Abstract
Background: This analysis sought to determine the associations of the Foundation for the National Institutes of Health Sarcopenia Project criteria for weakness and low lean mass with likelihood for mobility impairment (gait speed ≤ 0.8 m/s) and mortality. Providing validity for these criteria is essential for research and clinical evaluation.
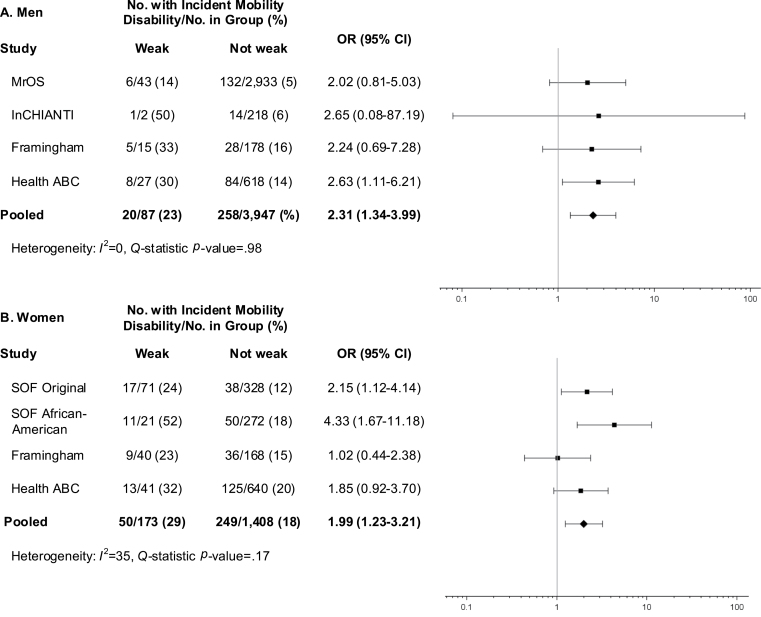
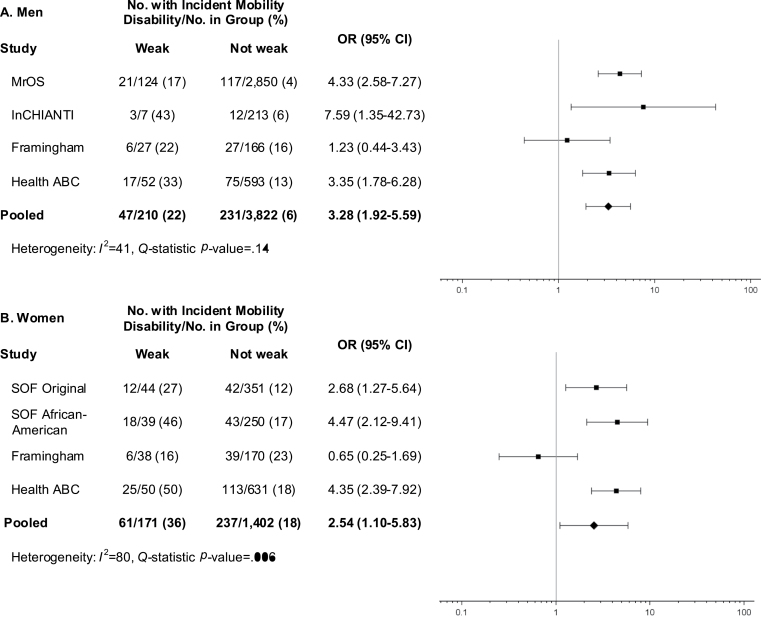
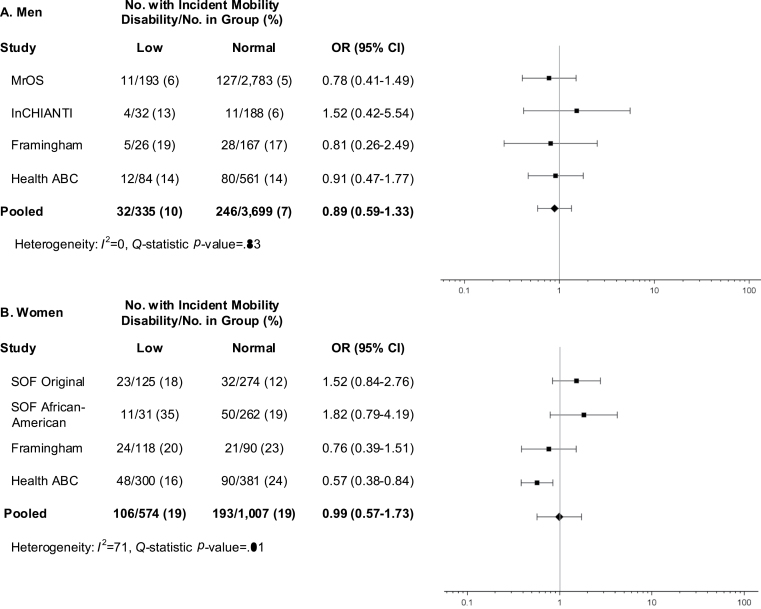
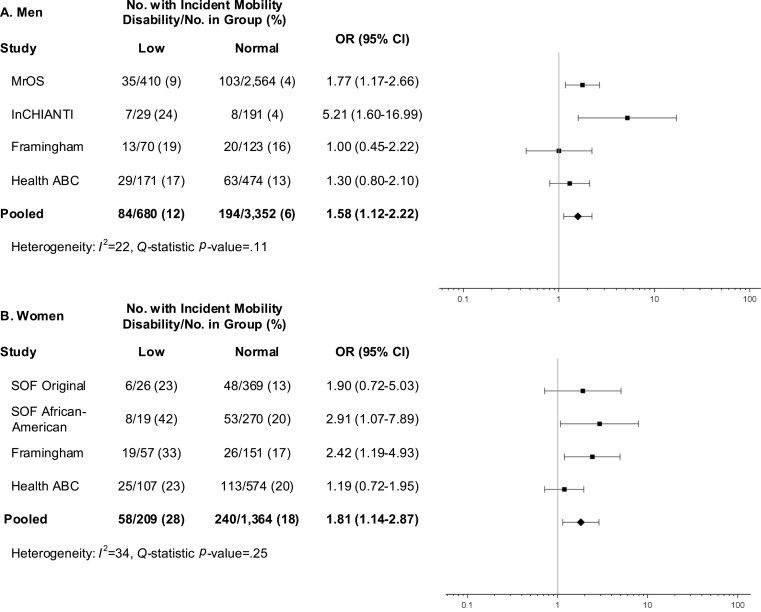
Methods: Among 4,411 men and 1,869 women pooled from 6 cohort studies, 3-year likelihood for incident mobility impairment and mortality over 10 years were determined for individuals with weakness, low lean mass, and for those having both. Weakness was defined as low grip strength (<26kg men and <16kg women) and low grip strength-to-body mass index (BMI; kg/m(2)) ratio (<1.00 men and <0.56 women). Low lean mass (dual-energy x-ray absorptiometry) was categorized as low appendicular lean mass (ALM; <19.75kg men and <15.02kg women) and low ALM-to-BMI ratio (<0.789 men and <0.512 women).
Results: Low grip strength (men: odds ratio [OR] = 2.31, 95% confidence interval [CI] = 1.34-3.99; women: OR = 1.99, 95% CI 1.23-3.21), low grip strength-to-BMI ratio (men: OR = 3.28, 95% CI 1.92-5.59; women: OR = 2.54, 95% CI 1.10-5.83) and low ALM-to-BMI ratio (men: OR = 1.58, 95% CI 1.12-2.25; women: OR = 1.81, 95% CI 1.14-2.87), but not low ALM, were associated with increased likelihood for incident mobility impairment. Weakness increased likelihood of mobility impairment regardless of low lean mass. Mortality risk patterns were inconsistent.
Conclusions: These findings support our cut-points for low grip strength and low ALM-to-BMI ratio as candidate criteria for clinically relevant weakness and low lean mass. Further validation in other populations and for alternate relevant outcomes is needed.
Keywords: Impairment.; Mobility; Muscle; Sarcopenia.
Figures
Similar articles
-
Cutpoints for low appendicular lean mass that identify older adults with clinically significant weakness.J Gerontol A Biol Sci Med Sci. 2014 May;69(5):567-75. doi: 10.1093/gerona/glu023. J Gerontol A Biol Sci Med Sci. 2014. PMID: 24737559 Free PMC article.
-
Putative Cut-Points in Sarcopenia Components and Incident Adverse Health Outcomes: An SDOC Analysis.J Am Geriatr Soc. 2020 Jul;68(7):1429-1437. doi: 10.1111/jgs.16517. Epub 2020 Jul 7. J Am Geriatr Soc. 2020. PMID: 32633824 Free PMC article.
-
Agreement and Predictive Validity Using Less-Conservative Foundation for the National Institutes of Health Sarcopenia Project Weakness Cutpoints.J Am Geriatr Soc. 2017 Mar;65(3):574-579. doi: 10.1111/jgs.14706. Epub 2016 Dec 26. J Am Geriatr Soc. 2017. PMID: 28024092 Free PMC article.
-
Assessment of Lean Mass and Physical Performance in Sarcopenia.J Clin Densitom. 2015 Oct-Dec;18(4):467-71. doi: 10.1016/j.jocd.2015.05.063. Epub 2015 Jun 10. J Clin Densitom. 2015. PMID: 26071168 Review.
-
Are sarcopenia and its individual components linked to all-cause mortality in heart failure? A systematic review and meta-analysis.Clin Res Cardiol. 2025 May;114(5):532-540. doi: 10.1007/s00392-023-02360-8. Epub 2023 Dec 12. Clin Res Cardiol. 2025. PMID: 38085294 Free PMC article.
Cited by
-
Association of Physical Activity and Exercise with Physical Performance and Muscle Mass in Older Adults: Results from the Longevity Check-Up (Lookup) 7+ Project.J Clin Med. 2023 Dec 5;12(24):7521. doi: 10.3390/jcm12247521. J Clin Med. 2023. PMID: 38137590 Free PMC article.
-
Sarcopenia and sarcopenic obesity: do they predict inferior oncologic outcomes after gastrointestinal cancer surgery?Perioper Med (Lond). 2016 Oct 26;5:30. doi: 10.1186/s13741-016-0052-1. eCollection 2016. Perioper Med (Lond). 2016. PMID: 27800156 Free PMC article. Review.
-
Sarcopenia, frailty and mortality: the evidence is growing.Age Ageing. 2016 Sep;45(5):570-1. doi: 10.1093/ageing/afw148. Age Ageing. 2016. PMID: 27609203 Free PMC article. No abstract available.
-
Causal associations of hand grip strength with bone mineral density and fracture risk: A mendelian randomization study.Front Endocrinol (Lausanne). 2022 Dec 12;13:1020750. doi: 10.3389/fendo.2022.1020750. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36578964 Free PMC article.
-
Handgrip Strength and Health in Aging Adults.Sports Med. 2018 Sep;48(9):1993-2000. doi: 10.1007/s40279-018-0952-y. Sports Med. 2018. PMID: 29943230
References
-
- Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr. 1997;127:990S–991S - PubMed
-
- Baumgartner RN, Koehler KM, Gallagher D, et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol. 1998;147:755–763 - PubMed
-
- Melton LJ, 3rd, Khosla S, Crowson CS, O’Connor MK, O’Fallon WM, Riggs BL. Epidemiology of sarcopenia. J Am Geriatr Soc. 2000;48:625–630 - PubMed
-
- Lauretani F, Russo CR, Bandinelli S, et al. Age-associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol. 2003;95:1851–1860 - PubMed
-
- Visser M, Goodpaster BH, Kritchevsky SB, et al. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J Gerontol A Biol Sci Med Sci. 2005;60:324–333 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
