

Costs and benefits of an organized fecal immunochemical test-based colorectal cancer screening program in the United States
- PMID: 24737634
- PMCID: PMC4593052
- DOI: 10.1002/cncr.28724
Costs and benefits of an organized fecal immunochemical test-based colorectal cancer screening program in the United States
Abstract
Background: Despite clear recommendations and evidence linking colorectal cancer screening to lower incidence and mortality, > 40% of adults are not up to date with screening. Existing domestic and international models of organized cancer screening programs have been effective in increasing screening rates. Implementing an organized, evidence-based, national screening program may be an effective approach to increasing screening rates.
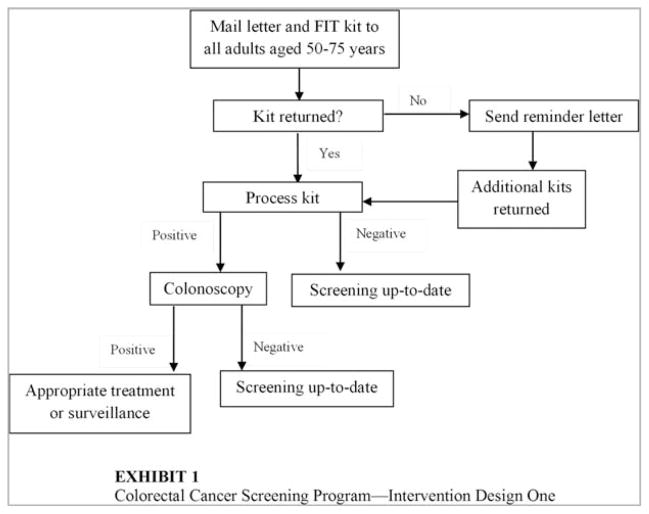
Methods: In the current study, the authors estimated the initial investment required and the cost per person screened of a nationwide fecal immunochemical test (FIT)-based colorectal cancer screening program among adults aged 50 years to 75 years.
Results: The initial additional investment required was estimated at $277.9 to $318.2 million annually, with an estimated 8.7 to 9.4 million individuals screened at a cost of $32 to $39 per person screened. The program was estimated to prevent 2900 to 3100 deaths annually.
Conclusions: The results of the current study indicate that implementing a national screening program would make a substantial public health impact at a moderate cost per person screened. Results from this analysis may provide useful information for understanding the public health benefit of an organized screening delivery system and the potential resources required to implement a nationwide colorectal cancer screening program, and help guide decisions about program planning, design, and implementation.
Keywords: colorectal cancer; early detection; health economics; public health; screening.
© 2014 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
Dr. Pignone’s work on the current study was supported by an Inter-agency Personnel Agreement with the Centers for Disease Control and Prevention.
Figures

Similar articles
-
Cost-effectiveness of colorectal cancer screening programmes using sigmoidoscopy and immunochemical faecal occult blood test.J Med Screen. 2019 Jun;26(2):76-83. doi: 10.1177/0969141318789710. Epub 2018 Sep 4. J Med Screen. 2019. PMID: 30180780
-
The Costs and Benefits of Risk Stratification for Colorectal Cancer Screening Based On Phenotypic and Genetic Risk: A Health Economic Analysis.Cancer Prev Res (Phila). 2021 Aug;14(8):811-822. doi: 10.1158/1940-6207.CAPR-20-0620. Epub 2021 May 26. Cancer Prev Res (Phila). 2021. PMID: 34039685 Free PMC article.
-
Cost-effectiveness and budget impact analyses of colorectal cancer screenings in a low- and middle-income country: example from Thailand.J Med Econ. 2019 Dec;22(12):1351-1361. doi: 10.1080/13696998.2019.1674065. Epub 2019 Oct 12. J Med Econ. 2019. PMID: 31560247
-
Screening for colorectal cancer: current status in Japan.Dis Colon Rectum. 2000 Oct;43(10 Suppl):S78-84. doi: 10.1007/BF02237230. Dis Colon Rectum. 2000. PMID: 11052482 Review.
-
Cost-effectiveness of Leveraging Social Determinants of Health to Improve Breast, Cervical, and Colorectal Cancer Screening: A Systematic Review.JAMA Oncol. 2020 Sep 1;6(9):1434-1444. doi: 10.1001/jamaoncol.2020.1460. JAMA Oncol. 2020. PMID: 32556187 Free PMC article.
Cited by
-
Editorial: Financial Incentives to Improve Colorectal Cancer Screening: Does it Make Cents?Am J Gastroenterol. 2016 Nov;111(11):1637-1639. doi: 10.1038/ajg.2016.459. Am J Gastroenterol. 2016. PMID: 27808152
-
Cost-Effectiveness of Community-to-Clinic Tailored Navigation for Colorectal Cancer Screening in an Underserved Population: Economic Evaluation Alongside a Group-Randomized Trial.Am J Health Promot. 2022 May;36(4):678-686. doi: 10.1177/08901171211068454. Epub 2022 Jan 27. Am J Health Promot. 2022. PMID: 35081762 Free PMC article. Clinical Trial.
-
Mailed fecal immunochemical test outreach for colorectal cancer screening: Summary of a Centers for Disease Control and Prevention-sponsored Summit.CA Cancer J Clin. 2020 Jul;70(4):283-298. doi: 10.3322/caac.21615. Epub 2020 Jun 25. CA Cancer J Clin. 2020. PMID: 32583884 Free PMC article.
-
Selection of patients for large mailed fecal immunochemical test colorectal cancer screening outreach programs: A systematic review.J Med Screen. 2021 Dec;28(4):379-388. doi: 10.1177/0969141321997482. Epub 2021 Mar 8. J Med Screen. 2021. PMID: 33683155 Free PMC article.
-
Modeling and Control of Colorectal Cancer.PLoS One. 2016 Aug 18;11(8):e0161349. doi: 10.1371/journal.pone.0161349. eCollection 2016. PLoS One. 2016. PMID: 27536786 Free PMC article.
References
-
- US Cancer Statistics Working Group. United States Cancer Statistics: 1999–2010 Incidence and Mortality Web-based Report. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; 2013. [Accessed February 25, 2014]. www.cdc.gov/uscs.
-
- Ekwueme DU, Guy GP, Li C, Rim SH, Parelkar P, Chen SC. The health burden and economic costs of cutaneous melanoma mortality by race/ethnicity–United States, 2000 to 2006. J Am Acad Dermatol. 2011;65(5 suppl 1):S133–S143. - PubMed
-
- US Preventive Services Task Force. Screening for Colorectal Cancer. Rockville, MD: Agency for Healthcare Research and Quality; 2008. [Accessed March 2, 2013]. uspreventiveservicestaskforce.org/uspstf/uspscolo.htm.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
