

Risk stratification and prognostic performance of the predisposition, infection, response, and organ dysfunction (PIRO) scoring system in septic patients in the emergency department: a cohort study
- PMID: 24739219
- PMCID: PMC4056311
- DOI: 10.1186/cc13832
Risk stratification and prognostic performance of the predisposition, infection, response, and organ dysfunction (PIRO) scoring system in septic patients in the emergency department: a cohort study
Abstract
Introduction: The predisposition, infection, response and organ dysfunction (PIRO) staging system was designed as a stratification tool to deal with the inherent heterogeneity of septic patients. The present study was conducted to assess the performance of PIRO in predicting multiple organ dysfunction (MOD), intensive care unit (ICU) admission, and 28-day mortality in septic patients in the emergency department (ED), and to compare this scoring system with the Mortality in Emergency Department Sepsis (MEDS) and Acute Physiology and Chronic Health Evaluation (APACHE II) scores.
Methods: Consecutive septic patients (n = 680) admitted to the ED of Beijing Chao-Yang Hospital were enrolled. PIRO, MEDS, and APACHE II scores were calculated for each patient on ED arrival. Organ function was reassessed within 3 days of enrollment. All patients were followed up for 28 days. Outcome criteria were the development of MOD within 3 days, ICU admission or death within 28 days after enrollment. The predictive ability of the four components of PIRO was analyzed separately. Receiver operating characteristic (ROC) curve and logistic regression analysis were used to assess the prognostic and risk stratification value of the scoring systems.
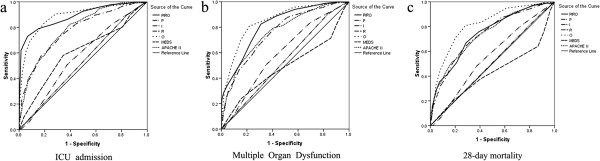
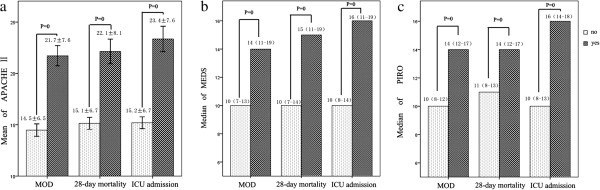
Results: Organ dysfunction independently predicted ICU admission, MOD, and 28-day mortality, with areas under the ROC curve (AUC) of 0.888, 0.851, and 0.816, respectively. The predictive value of predisposition, infection, and response was weaker than that of organ dysfunction. A negative correlation was found between the response component and MOD, as well as mortality. PIRO, MEDS, and APACHE II scores significantly differed between patients who did and did not meet the outcome criteria (P < 0.001). PIRO and APACHE II independently predicted ICU admission and MOD, but MEDS did not. All three systems were independent predictors of 28-day mortality with similar AUC values. The AUC of PIRO was 0.889 for ICU admission, 0.817 for MOD, and 0.744 for 28-day mortality. The AUCs of PIRO were significantly greater than those of APACHE II and MEDS (P < 0.05) in predicting ICU admission and MOD.
Conclusions: The study indicates that PIRO is helpful for risk stratification and prognostic determinations in septic patients in the ED.
Figures
Similar articles
-
Predictive Value of Combination of Procalcitonin and Predisposition, Infection, Response, and Organ Dysfunction (PIRO) System in Septic Patients with Positive Blood Cultures in the Emergency Department.Infect Drug Resist. 2022 Oct 26;15:6189-6202. doi: 10.2147/IDR.S384689. eCollection 2022. Infect Drug Resist. 2022. PMID: 36312440 Free PMC article.
-
Comparison of Predisposition, Insult/Infection, Response, and Organ dysfunction, Acute Physiology And Chronic Health Evaluation II, and Mortality in Emergency Department Sepsis in patients meeting criteria for early goal-directed therapy and the severe sepsis resuscitation bundle.J Crit Care. 2012 Aug;27(4):362-9. doi: 10.1016/j.jcrc.2011.08.013. Epub 2011 Oct 26. J Crit Care. 2012. PMID: 22033054
-
Sepsis patients in the emergency department: stratification using the Clinical Impression Score, Predisposition, Infection, Response and Organ dysfunction score or quick Sequential Organ Failure Assessment score?Eur J Emerg Med. 2018 Oct;25(5):328-334. doi: 10.1097/MEJ.0000000000000460. Eur J Emerg Med. 2018. PMID: 28338533 Free PMC article.
-
Scoring Systems for Organ Dysfunction and Multiple Organ Dysfunction: The PODIUM Consensus Conference.Pediatrics. 2022 Jan 1;149(1 Suppl 1):S23-S31. doi: 10.1542/peds.2021-052888D. Pediatrics. 2022. PMID: 34970683 Free PMC article.
-
Performance of early warning and risk stratification scores versus clinical judgement in the acute setting: a systematic review.Emerg Med J. 2022 Dec;39(12):918-923. doi: 10.1136/emermed-2021-211524. Epub 2022 Aug 9. Emerg Med J. 2022. PMID: 35944968
Cited by
-
Prevalence of organ failure and mortality among patients in the emergency department: a population-based cohort study.BMJ Open. 2019 Oct 30;9(10):e032692. doi: 10.1136/bmjopen-2019-032692. BMJ Open. 2019. PMID: 31666275 Free PMC article.
-
Predisposition, Insult, Response, and Organ Dysfunction: A Well-constructed Score!Indian J Crit Care Med. 2023 Feb;27(2):150. doi: 10.5005/jp-journals-10071-24401. Indian J Crit Care Med. 2023. PMID: 36865520 Free PMC article.
-
Systematic screening is essential for early diagnosis of severe sepsis and septic shock.Rev Bras Ter Intensiva. 2015 Apr-Jun;27(2):96-101. doi: 10.5935/0103-507X.20150018. Rev Bras Ter Intensiva. 2015. PMID: 26340147 Free PMC article. No abstract available.
-
Machine Learning Model Development and Validation for Predicting Outcome in Stage 4 Solid Cancer Patients with Septic Shock Visiting the Emergency Department: A Multi-Center, Prospective Cohort Study.J Clin Med. 2022 Dec 5;11(23):7231. doi: 10.3390/jcm11237231. J Clin Med. 2022. PMID: 36498805 Free PMC article.
-
Predictive Value of Combination of Procalcitonin and Predisposition, Infection, Response, and Organ Dysfunction (PIRO) System in Septic Patients with Positive Blood Cultures in the Emergency Department.Infect Drug Resist. 2022 Oct 26;15:6189-6202. doi: 10.2147/IDR.S384689. eCollection 2022. Infect Drug Resist. 2022. PMID: 36312440 Free PMC article.
References
-
- Vincent JL, Sakr Y, Sprung CL, Ranieri VM, Reinhart K, Gerlach H, Moreno R, Carlet J, Le Gall JR, Payen D. Sepsis Occurrence in Acutely Ill Patients Investigators. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34:344–353. doi: 10.1097/01.CCM.0000194725.48928.3A. - DOI - PubMed
-
- Moerer O, Schmid A, Hofmann M, Herklotz A, Reinhart K, Werdan K, Schneider H, Burchardi H. Direct costs of severe sepsis in three German intensive care units based on retrospective electronic patient record analysis of resource use. Intensive Care Med. 2002;28:1440–1446. doi: 10.1007/s00134-002-1429-9. - DOI - PubMed
-
- Esteban A, Frutos-Vivar F, Ferguson ND, Peñuelas O, Lorente JA, Gordo F, Honrubia T, Algora A, Bustos A, García G, Diaz-Regañón IR, de Luna RR. Sepsis incidence and outcome: contrasting the intensive care unit with the hospital ward. Crit Care Med. 2007;35:1284–1289. doi: 10.1097/01.CCM.0000260960.94300.DE. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
