

The differential diagnosis and treatment of tremor
- PMID: 24739887
- PMCID: PMC3991161
- DOI: 10.3238/arztebl.2014.0225
The differential diagnosis and treatment of tremor
Abstract
Background: Essential tremor is the most common type of tremor, with a prevalence of 0.4% in the overall population and 4-7% in persons over age 65. In general, tremor is so common that patients with tremor are frequently treated not only by neurologists, but also by physicians from other specialties.
Method: This review is based on publications retrieved by a selective PubMed search and on guidelines from Germany and abroad.
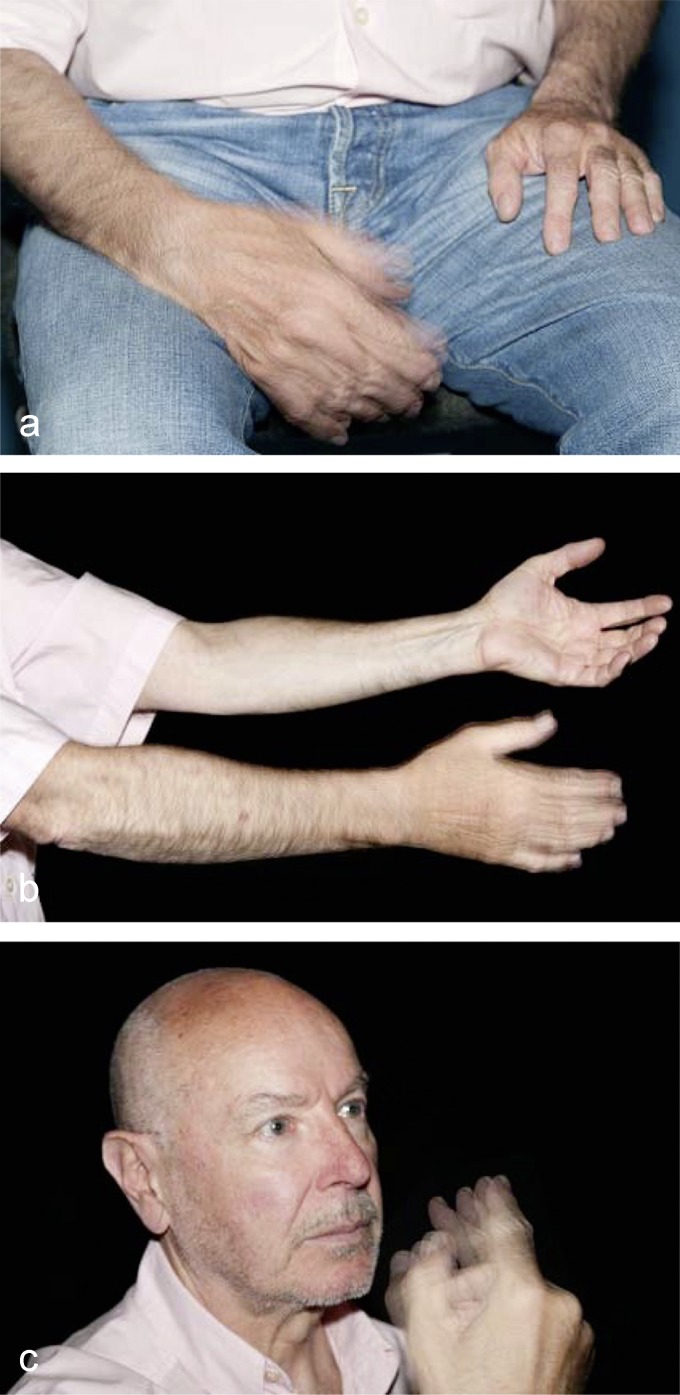
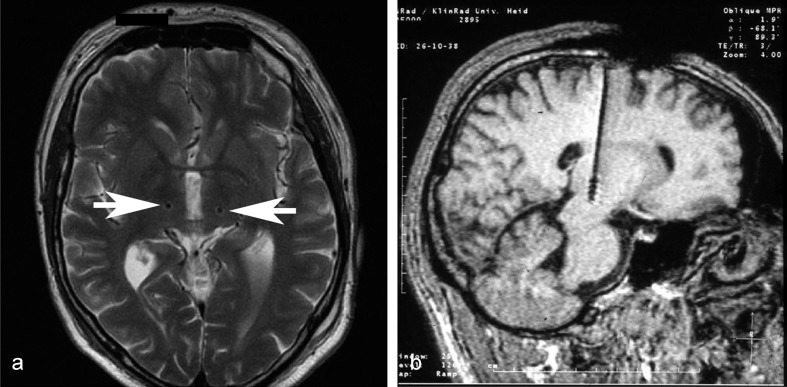
Results: Particular tremor syndromes are usually diagnosed on the basis of their typical clinical presentation and whatever accompanying manifestations may be present. Ancillary tests are usually unnecessary. Unilateral rest tremor accompanied by rigidity and bradykinesia is typical of Parkinson's disease. Essential tremor is a bilateral postural tremor. The most common cause of intention tremor is multiple sclerosis. Mild tremor syndromes can often be treated satisfactorily with drugs. In case of severe tremor, which is rarer, a stereotactic operation can be considered. The usual outcome of such procedures is the complete suppression of tremor.
Conclusion: Most patients with tremor can be given a precise diagnosis and offered specific treatment. It is important for the physician to inform the patient about the expected course of tremor over time, its possible genetic causes, and the various available treatments.
Figures
References
-
- Deuschl G, Bain P, Brin M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov Disord. 1998;13(Suppl 3 M):2–23. - PubMed
-
- Schulz JB, Gasser T. Parkinson-Syndrome. In: Brandt T, Diener HC, Gerloff C, editors. Therapie und Verlauf neurologischer Erkrankungen. Stuttgart: Kohlhammer; 2012. pp. p. 943–988.
-
- Ebersbach G, Stoeck M, Müller J, Wissel J, Poewe W. Dopa-responsiver Haltetremor bei idiopathischer Parkinson Erkrankung. Aktuelle Neurologie. 2000;27:327–331.
-
- Reichmann H. Budipine in Parkinson’s tremor. J Neurol Sci. 2006;248:53–55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical