

Altered lower extremity fracture characteristics in obese pediatric trauma patients
- PMID: 24740109
- PMCID: PMC4198524
- DOI: 10.1097/BOT.0000000000000132
Altered lower extremity fracture characteristics in obese pediatric trauma patients
Abstract
Objective: To determine whether there are differences in fracture patterns and femur fracture treatment choices in obese versus nonobese pediatric trauma patients.
Design: Prognostic study, retrospective chart review.
Setting: Two level I pediatric trauma centers.
Patients: The trauma registries of 2 pediatric hospitals were queried for patients with lower extremity long-bone fractures resulting from blunt trauma. 2858 alerts were examined, and 397 patients had lower extremity fractures. Three hundred thirty-one patients with a total of 394 femur or tibia fractures met the inclusion criteria, and 70 patients (21%) were obese.
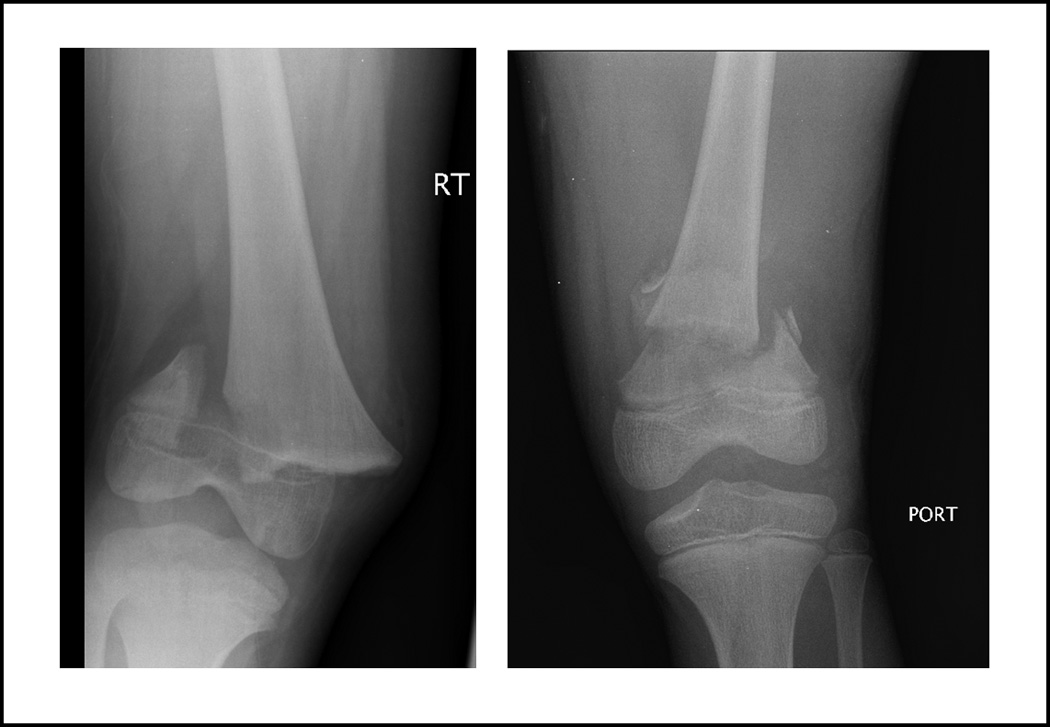
Main outcome measurements: Weight for age >95th percentile was defined as obese. Radiographs were reviewed, and fractures were classified according the OTA/AO pediatric fracture classification system. Fracture patterns (OTA subsegment), severity, and choice of intervention for femur fractures were the primary outcomes.
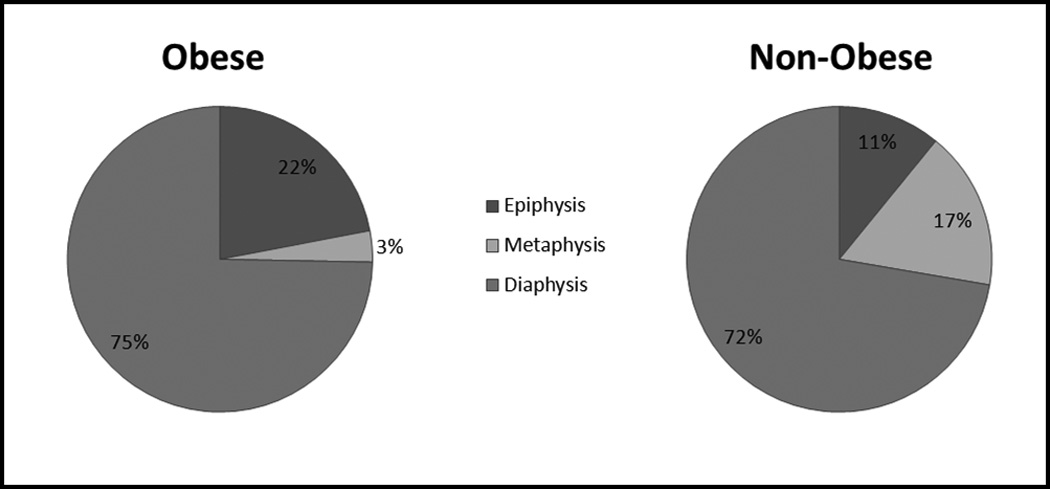
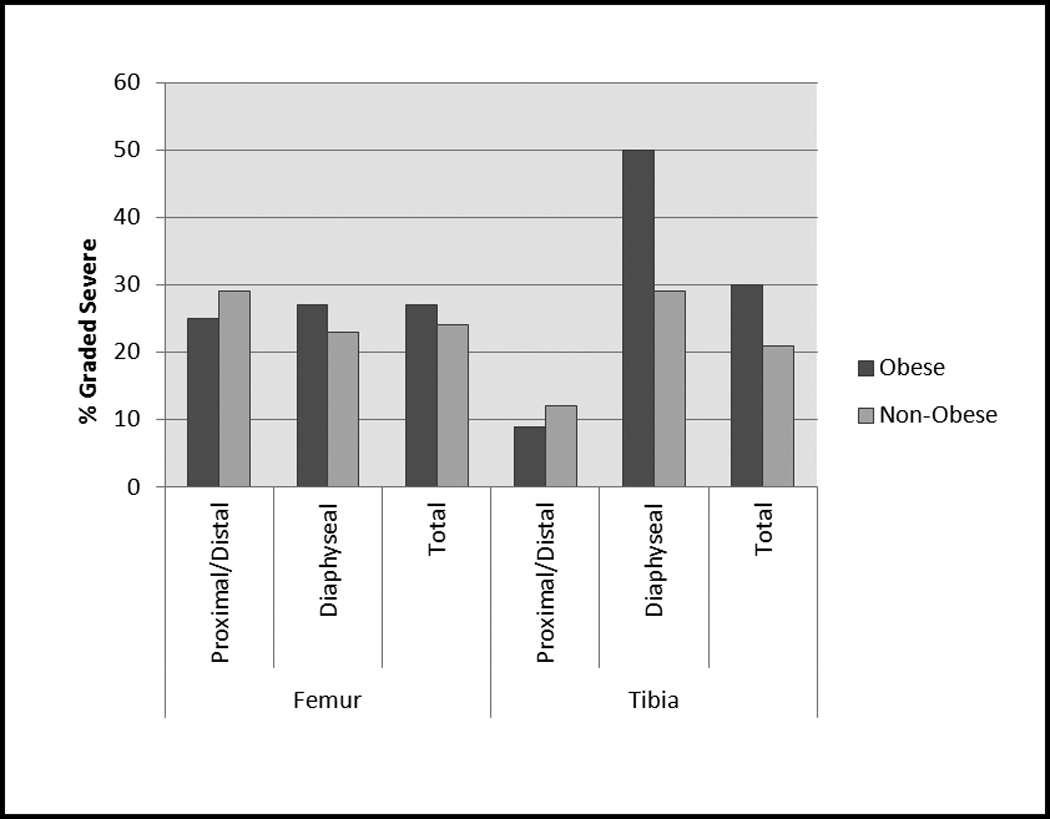
Results: Overall, obese patients were twice as likely [risk ratio (RR), 2.20; 95% confidence interval (CI), 1.25-3.89] to have fractures involving the physis. Physeal fracture risk was greater for femur fractures (RR, 3.25; 95% CI, 1.35-7.78) than tibia fractures (RR, 1.58; 95% CI, 0.76-3.26). Severity did not differ between groups. Obese patients with femur fractures were more likely to be treated with locked nails.
Conclusions: Obese pediatric trauma patients are more likely to sustain fractures involving the physis than nonobese patients. This could be related to intrinsic changes to the physis related to obesity or altered biomechanical forces. This is consistent with the observed relationships between obesity and other conditions affecting the physis including Blount disease and slipped capital femoral epiphysis.
Level of evidence: Prognostic Level II. See Instructions for Authors for a complete description of levels of evidence.
Conflict of interest statement
Conflicts of interest: Aaron Creek and Jeffery Sawyer declare no conflicts of interest.
Figures
References
-
- Childhood Obesity Action Network. State Obesity Profiles, 2009. National Initiative for Children's Healthcare Quality Child Policy Research Center, and Child and Adolescent Health Measurement Initiative. from www.childhealthdata.org/browse/snapshots/obesity-2007.
-
- Dietz WH. Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics. 1998;101(3 Pt 2):518–525. - PubMed
-
- Gettys FK, Jackson JB, Frick SL. Obesity in pediatric orthopaedics. Orthop Clin North Am. 2011;42(1):95–105. vii. - PubMed
-
- Dimitri P, Wales JK, Bishop N. Fat and bone in children: differential effects of obesity on bone size and mass according to fracture history. J Bone Miner Res. 2010;25(3):527–536. - PubMed
-
- Dimitri P, Bishop N, Walsh JS, et al. Obesity is a risk factor for fracture in children but is protective against fracture in adults: A paradox. Bone. 2012;50(2):547–566. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
