

Association between diabetes mellitus and angina after acute myocardial infarction: analysis of the TRIUMPH prospective cohort study
- PMID: 24740679
- PMCID: PMC4199926
- DOI: 10.1177/2047487314533622
Association between diabetes mellitus and angina after acute myocardial infarction: analysis of the TRIUMPH prospective cohort study
Abstract
Aims: While patients with diabetes mellitus (DM) have more extensive coronary disease and worse survival after acute myocardial infarction (AMI) than patients without DM, data on whether they experience more angina are conflicting.
Methods: We examined angina prevalence over the year following AMI among 3367 patients, including 1080 (32%) with DM, from 24 US hospitals enrolled in the TRIUMPH registry from 2005 to 2008.
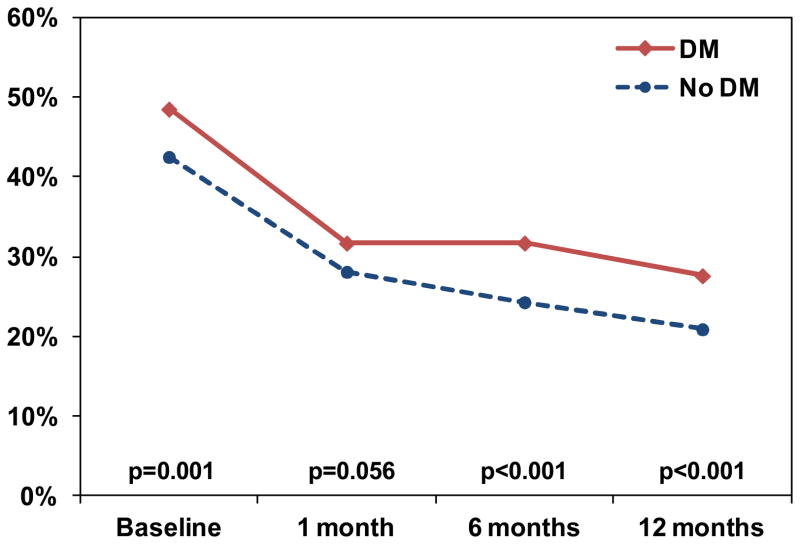
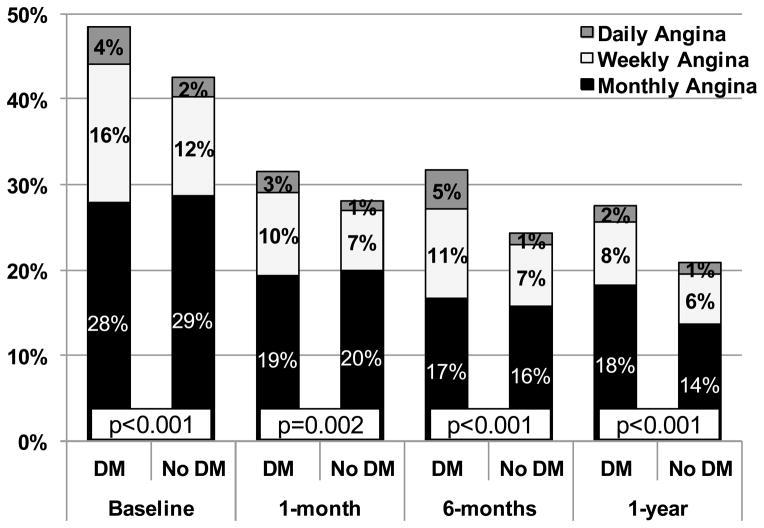
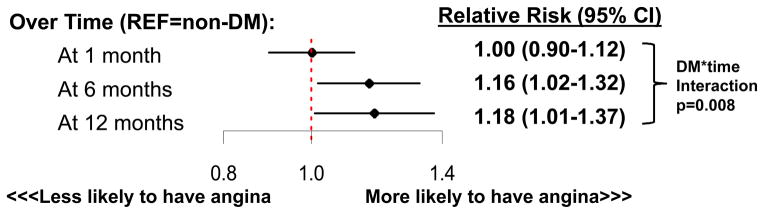
Results: Patients with vs. without DM were more likely to be treated with antianginal medications both at discharge and over follow up. Despite more aggressive angina therapy, patients with vs. without DM had higher prevalence and severity of angina prior to AMI (49 vs. 43%, p = 0.001) and at each follow-up assessment, although rates of angina declined in both groups over time. In a hierarchical, multivariable, repeated-measures model that adjusted for multiple demographic and clinical factors including severity of coronary disease and in-hospital revascularization, DM was associated with a greater odds of angina over the 12 months of follow up; this association increased in magnitude over time (12-month OR 1.18, 95% CI 1.01-1.37; DM*time pinteraction = 0.008).
Conclusions: Contrary to conventional wisdom, angina is more prevalent and more severe among patients with DM, both prior to and following AMI. This effect is amplified over time and independent of patient and treatment factors, including the presence of multivessel disease and coronary revascularization. This increased burden of angina may be due to more diffuse nature of coronary disease, more rapid progression of coronary disease over time, or greater myocardial demand among DM patients.
Keywords: Angina; diabetes mellitus; myocardial infarction.
© The European Society of Cardiology 2014 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav.
Conflict of interest statement
The other authors report no conflicts of interest.
Figures
References
-
- Abi Khalil C, Roussel R, Mohammedi K, Danchin N, Marre M. Cause-specific mortality in diabetes: recent changes in trend mortality. Eur J Prev Cardiol. 2012;19(3):374–81. - PubMed
-
- Donahoe SM, Stewart GC, McCabe CH, Mohanavelu S, Murphy SA, Cannon CP, Antman EM. Diabetes and mortality following acute coronary syndromes. JAMA. 2007;298(7):765–75. - PubMed
-
- Duarte R, Castela S, Reis RP, Correia MJ, Ramos A, Pereira AP, Martins P, Correia JM. Acute coronary syndrome in a diabetic population--risk factors and clinical and angiographic characteristics. Rev Port Cardiol. 2003;22(9):1077–88. - PubMed
-
- Herlitz J, Wognsen GB, Emanuelsson H, Haglid M, Karlson BW, Karlsson T, Albertsson P, Westberg S. Mortality and morbidity in diabetic and nondiabetic patients during a 2-year period after coronary artery bypass grafting. Diabetes Care. 1996;19(7):698–703. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
