

Tubercular spondylitis in children
- PMID: 24741133
- PMCID: PMC3977367
- DOI: 10.4103/0019-5413.128747
Tubercular spondylitis in children
Abstract
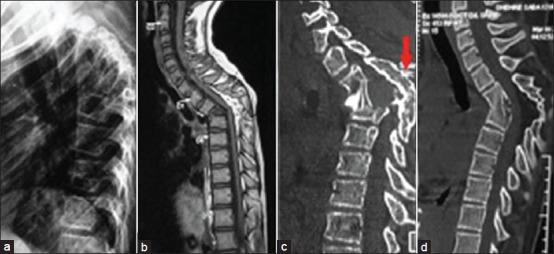
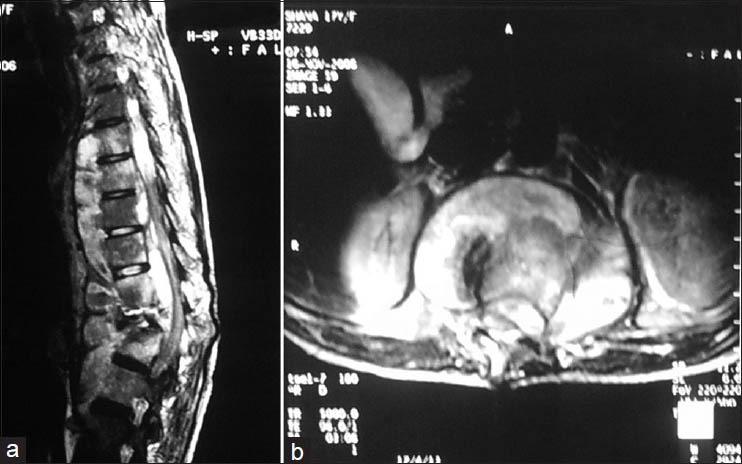
Spine of the child has unique anatomy and growth potential to grow to adult size. Tuberculosis (TB) spine results in bone loss as well as disturbed growth potential, hence spinal deformities may progress as the child grows. The growth potential is also disturbed when the disease focus is surgically intervened. Surgery is indicated for complications such as deformity, neurological deficit, instability, huge abscess, diagnostic dilemma and in suspected drug resistance to mycobacterium tuberculosis. The child on antitubercular treatment needs to be periodically evaluated for weight gain and drug dosages need to be adjusted accordingly. The severe progressive kyphotic deformity should be surgically corrected. Mild to moderate cases should be followed up until maturity to observe progression/improvement of spinal deformity. The surgical correction of kyphotic deformity in active disease is less hazardous than in a healed kyphosis. The internal kyphectomy by extra pleural approach allows adequate removal of internal salient in paraplegic patients with healed kyphotic deformity.
Keywords: Kyphus correction; osteoarticular tuberculosis; pediatric tuberculosis; tuberculosis of spine.
Conflict of interest statement
Figures


References
-
- Sarwark J, Aubin CE. Growth considerations of the immature spine. J Bone Joint Surg Am. 2007;89:8–13. - PubMed
-
- Soames RW. Skeletal system. In: Williams LH, Berry MM, Collins P, Dyson M, Dussek J, Ferguson MW, editors. Gray's Anatomy: The Anatomical Basis of Medicine and Surgery. 38th ed. New York: Churchill Livingstone; 1995. pp. 510–36.
-
- Dimeglio A, Ferran JL. Three-dimensional analysis of the hip during growth. Acta Orthop Belg. 1990;56:111–4. - PubMed
-
- Roaf R. Vertebral growth and its mechanical control. J Bone Joint Surg Br. 1960;42-B:40–59. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources