

Diffusion tensor imaging for outcome prediction in mild traumatic brain injury: a TRACK-TBI study
- PMID: 24742275
- PMCID: PMC4144386
- DOI: 10.1089/neu.2013.3171
Diffusion tensor imaging for outcome prediction in mild traumatic brain injury: a TRACK-TBI study
Abstract
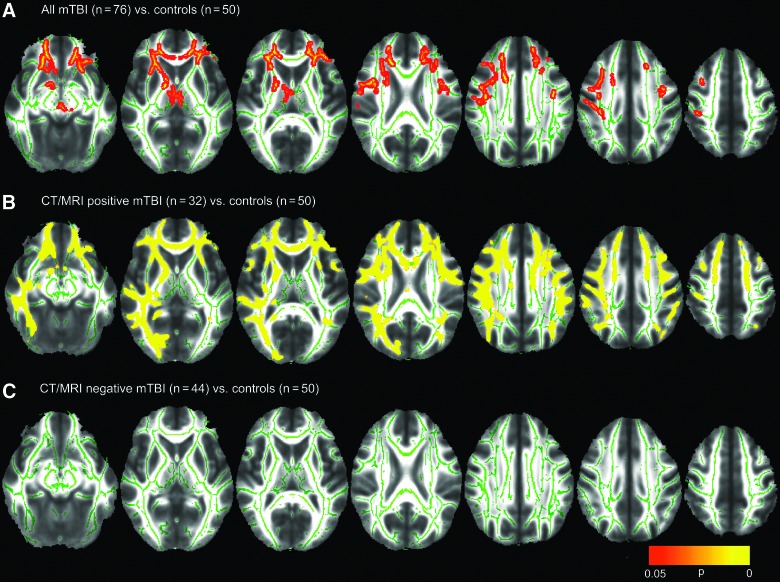
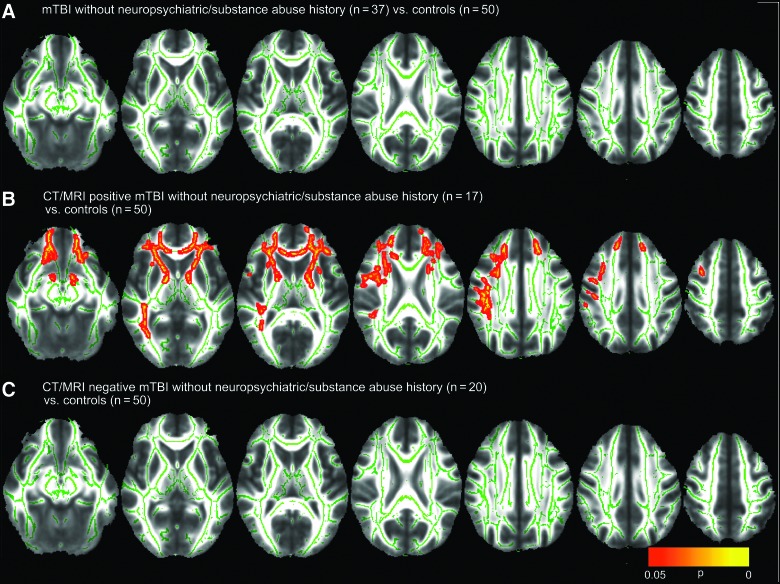
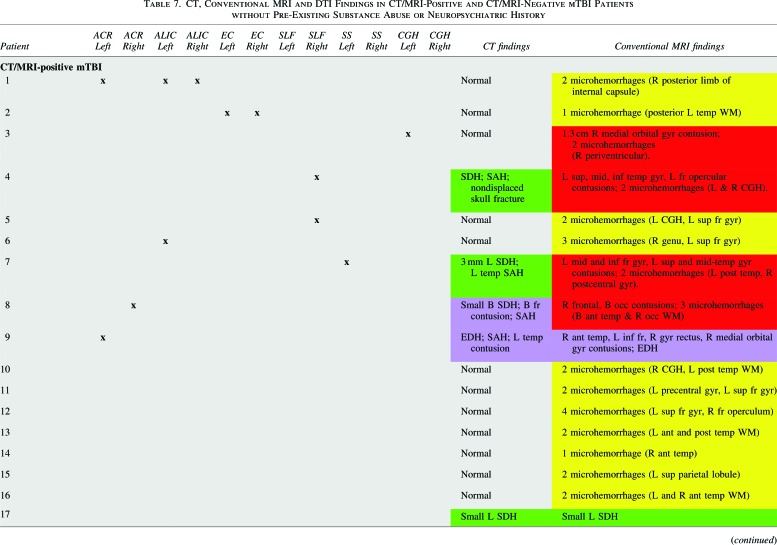
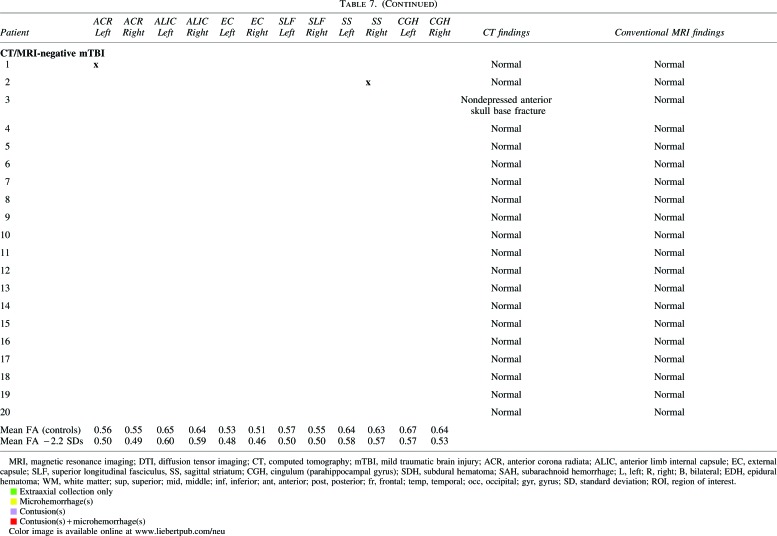
We evaluated 3T diffusion tensor imaging (DTI) for white matter injury in 76 adult mild traumatic brain injury (mTBI) patients at the semiacute stage (11.2±3.3 days), employing both whole-brain voxel-wise and region-of-interest (ROI) approaches. The subgroup of 32 patients with any traumatic intracranial lesion on either day-of-injury computed tomography (CT) or semiacute magnetic resonance imaging (MRI) demonstrated reduced fractional anisotropy (FA) in numerous white matter tracts, compared to 50 control subjects. In contrast, 44 CT/MRI-negative mTBI patients demonstrated no significant difference in any DTI parameter, compared to controls. To determine the clinical relevance of DTI, we evaluated correlations between 3- and 6-month outcome and imaging, demographic/socioeconomic, and clinical predictors. Statistically significant univariable predictors of 3-month Glasgow Outcome Scale-Extended (GOS-E) included MRI evidence for contusion (odds ratio [OR] 4.9 per unit decrease in GOS-E; p=0.01), ≥1 ROI with severely reduced FA (OR, 3.9; p=0.005), neuropsychiatric history (OR, 3.3; p=0.02), age (OR, 1.07/year; p=0.002), and years of education (OR, 0.79/year; p=0.01). Significant predictors of 6-month GOS-E included ≥1 ROI with severely reduced FA (OR, 2.7; p=0.048), neuropsychiatric history (OR, 3.7; p=0.01), and years of education (OR, 0.82/year; p=0.03). For the subset of 37 patients lacking neuropsychiatric and substance abuse history, MRI surpassed all other predictors for both 3- and 6-month outcome prediction. This is the first study to compare DTI in individual mTBI patients to conventional imaging, clinical, and demographic/socioeconomic characteristics for outcome prediction. DTI demonstrated utility in an inclusive group of patients with heterogeneous backgrounds, as well as in a subset of patients without neuropsychiatric or substance abuse history.
Keywords: axonal injury; computed tomography; diffusion tensor imaging; magnetic resonance imaging; traumatic brain injury.
Figures
References
-
- Faul M., Xu L., Wald M.M., and Coronado V.G. (2010). Traumatic brain injury in the United States: emergency department visits, hospitalizations, and deaths. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control: Atlanta, GA
-
- Mild Traumatic Brain Injury Committee. Head Injury Interdisciplinary Special Interest Group of the American Congress of Rehabilitation Medicine. (1993). Definition of mild traumatic brain injury. J. Head Trauma Rehabil. 8, 86–87
-
- National Center for Injury Prevention and Control. (2003). Report to Congress on mild traumatic brain injury in the United States: steps to prevent a serious public health problem. Centers for Disease Control and Prevention: Atlanta, GA
-
- Carroll L.J., Cassidy J.D., Holm L., Kraus J., and Coronado V.G.; WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. (2004). Methodological issues and research recommendations for mild traumatic brain injury: the WHO Collaborating Center Task Force on Mild Traumatic Brain Injury. J, Rehabil. Med. 43, Suppl., 113–125 - PubMed
-
- Bernstein D.M. (1999). Recovery from mild head injury. Brain Inj. 13, 151–172 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
