

Serum creatinine changes associated with critical illness and detection of persistent renal dysfunction after AKI
- PMID: 24742481
- PMCID: PMC4046736
- DOI: 10.2215/CJN.11141113
Serum creatinine changes associated with critical illness and detection of persistent renal dysfunction after AKI
Abstract
Background and objectives: AKI is a risk factor for development or worsening of CKD. However, diagnosis of renal dysfunction by serum creatinine could be confounded by loss of muscle mass and creatinine generation after critical illness.
Design, setting, participants, & measurements: A retrospective, single center analysis of serum in patients surviving to hospital discharge with an intensive care unit admission of 5 or more days between 2009 and 2011 was performed.
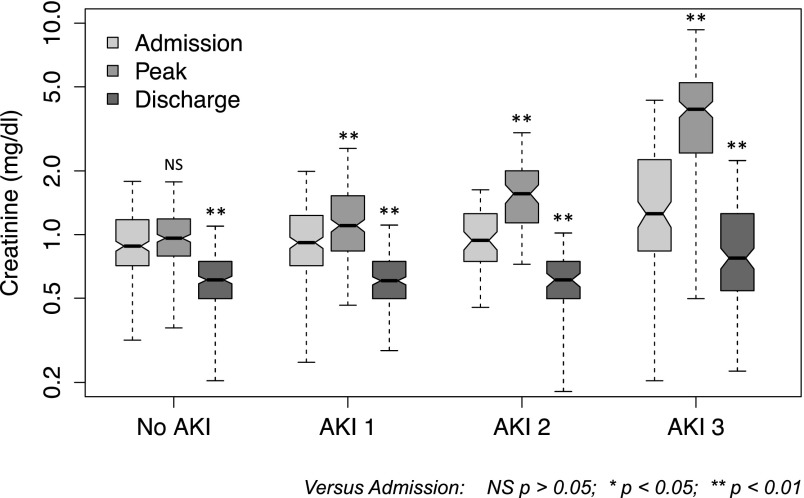
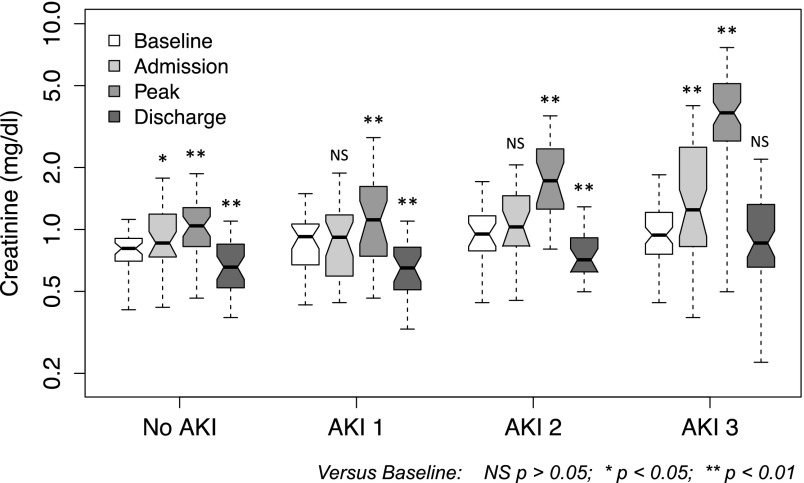
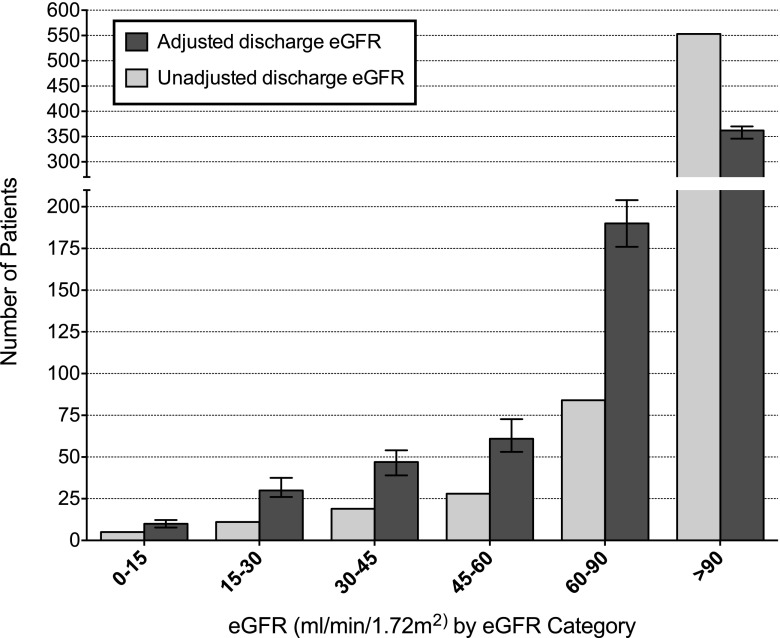
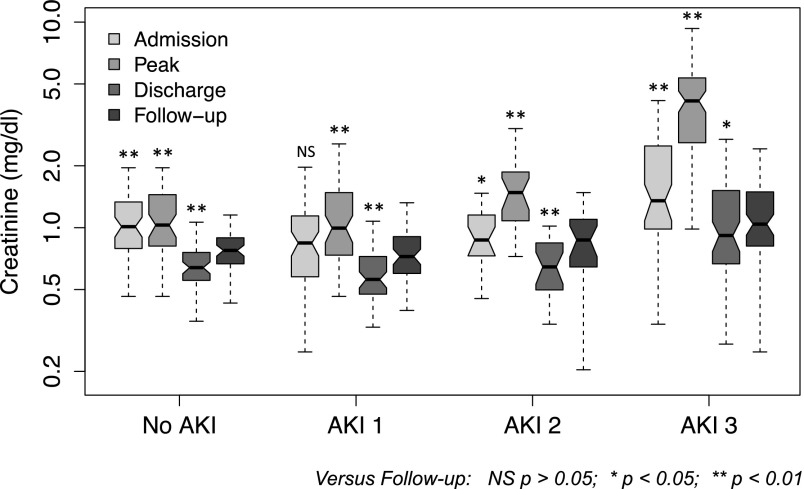
Results: In total, 700 cases were identified, with a 66% incidence of AKI. In 241 patients without AKI, creatinine was significantly lower (P<0.001) at hospital discharge than admission (median, 0.61 versus 0.88 mg/dl; median decrease, 33%). In 160 patients with known baseline, discharge creatinine was significantly lower than baseline in all patients except those patients with severe AKI (Kidney Disease Improving Global Outcomes category 3), who had no significant difference. In a multivariable regression model, median duration of hospitalization was associated with a predicted 30% decrease (95% confidence interval, 8% to 45%) in creatinine from baseline in the absence of AKI; after allowing for this effect, AKI was associated with a 29% (95% confidence interval, 10% to 51%) increase in predicted hospital discharge creatinine. Using a similar model to exclude the confounding effect of prolonged major illness on creatinine, 148 of 700 patients (95% confidence interval, 143 to 161) would have eGFR<60 ml/min per 1.73 m(2) at hospital discharge compared with only 63 of 700 patients using eGFR based on unadjusted hospital creatinine (a 135% increase in potential CKD diagnoses; P<0.001).
Conclusion: Critical illness is associated with significant falls in serum creatinine that persist to hospital discharge, potentially causing inaccurate assessment of renal function at discharge, particularly in survivors of AKI. Prospective measurements of GFR and creatinine generation are required to confirm the significance of these findings.
Keywords: acute renal failure; creatinine; glomerular filtration rate; progression of chronic renal failure.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Mehta RL, Pascual MT, Soroko S, Chertow GM, PICARD Study Group : Diuretics, mortality, and nonrecovery of renal function in acute renal failure. JAMA 288: 2547–2553, 2002 - PubMed
-
- Amdur RL, Chawla LS, Amodeo S, Kimmel PL, Palant CE: Outcomes following diagnosis of acute renal failure in U.S. veterans: Focus on acute tubular necrosis. Kidney Int 76: 1089–1097, 2009 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
