

Efficient phagocytosis and laccase activity affect the outcome of HIV-associated cryptococcosis
- PMID: 24743149
- PMCID: PMC4001551
- DOI: 10.1172/JCI72950
Efficient phagocytosis and laccase activity affect the outcome of HIV-associated cryptococcosis
Abstract
Background: Cryptococcal meningitis (CM) is a leading cause of HIV-associated mortality globally. High fungal burden in cerebrospinal fluid (CSF) at diagnosis and poor fungal clearance during treatment are recognized adverse prognostic markers; however, the underlying pathogenic factors that drive these clinical manifestations are incompletely understood. We profiled a large set of clinical isolates for established cryptococcal virulence traits to evaluate the contribution of C. neoformans phenotypic diversity to clinical presentation and outcome in human cryptococcosis.
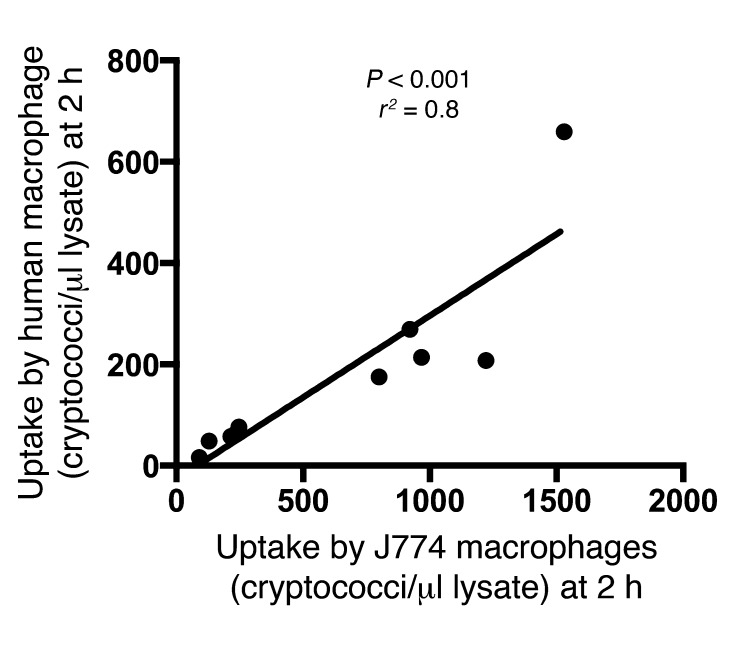
Methods: Sixty-five C. neoformans isolates from clinical trial patients with matched clinical data were assayed in vitro to determine murine macrophage uptake, intracellular proliferation rate (IPR), capsule induction, and laccase activity. Analysis of the correlation between prognostic clinical and host immune parameters and fungal phenotypes was performed using Spearman's r, while the fungal-dependent impact on long-term survival was determined by Cox regression analysis.
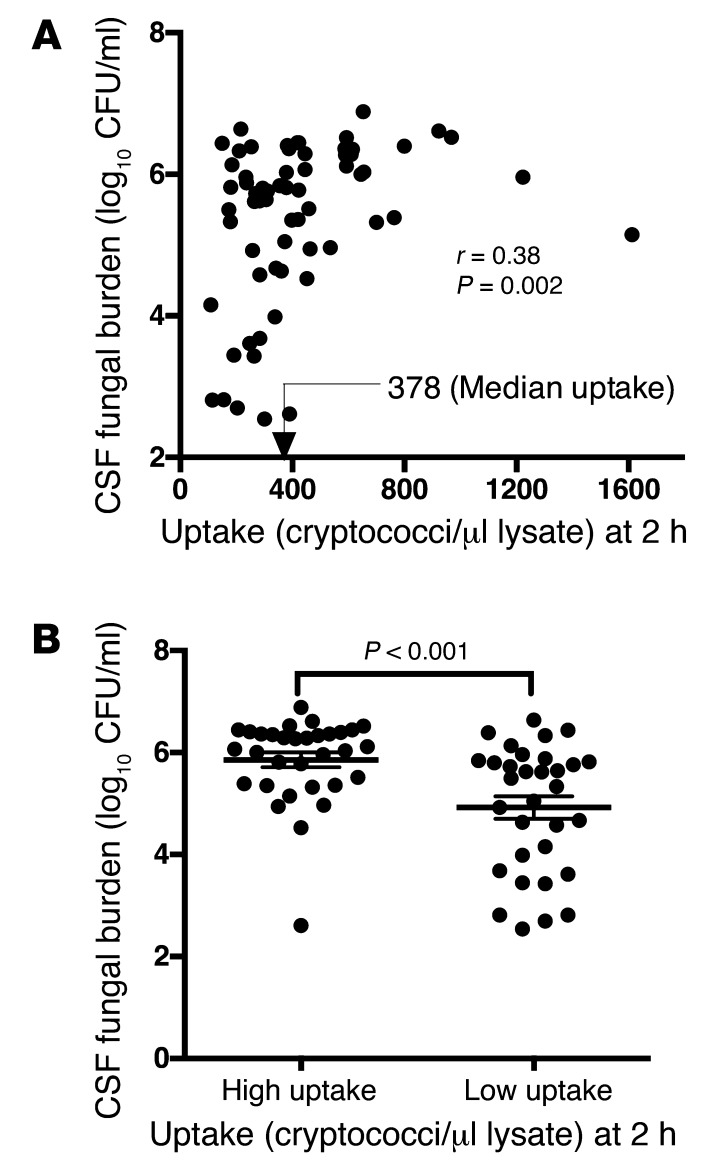
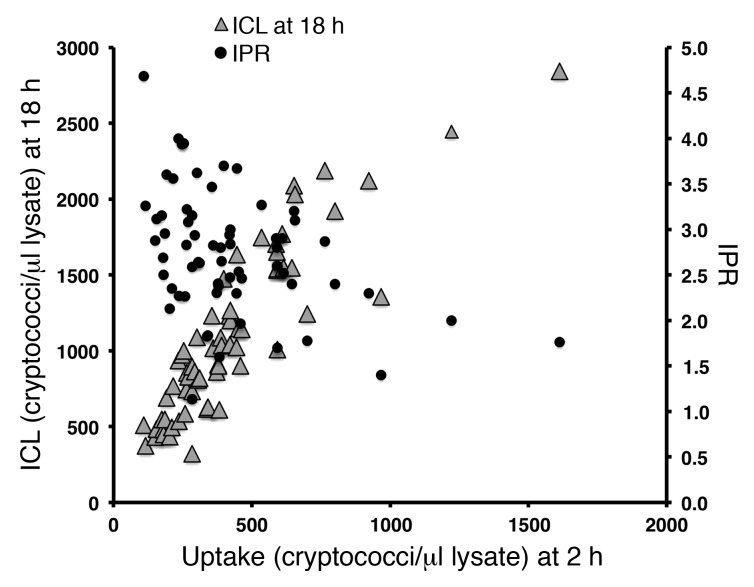
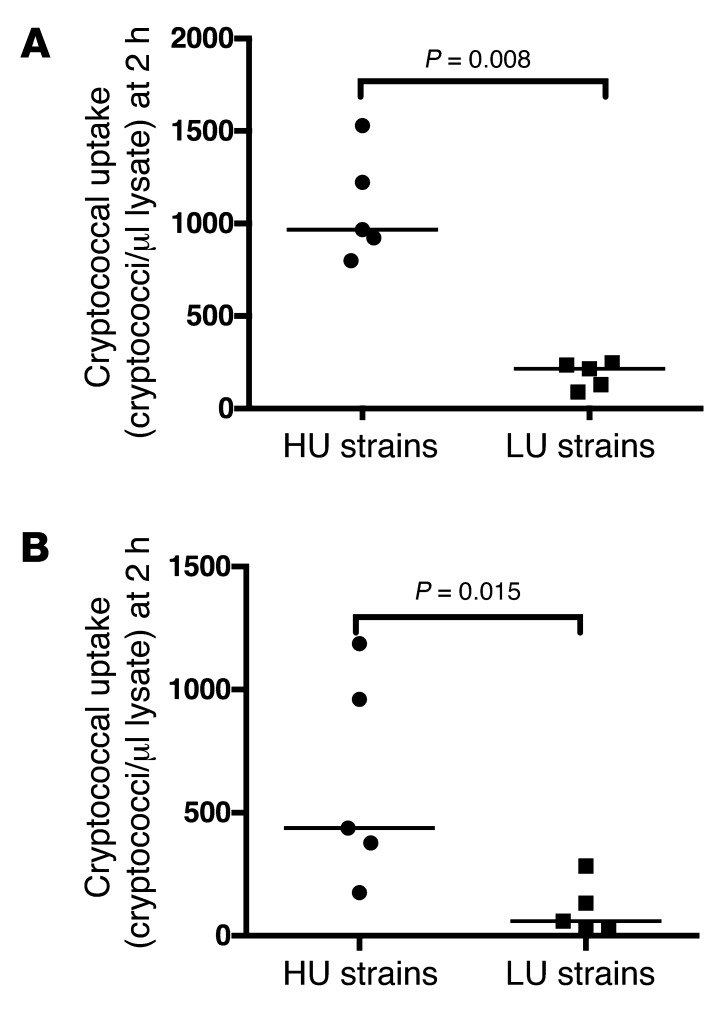
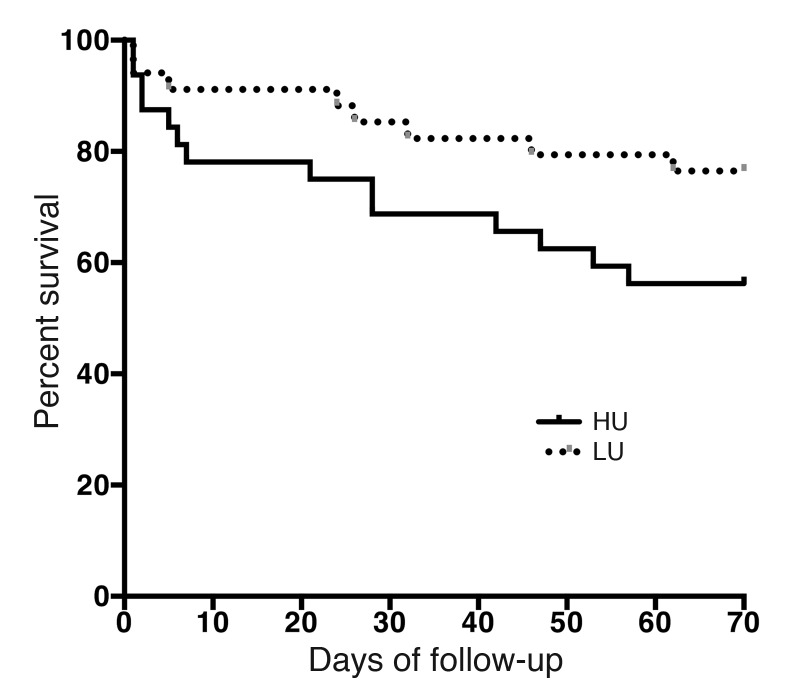
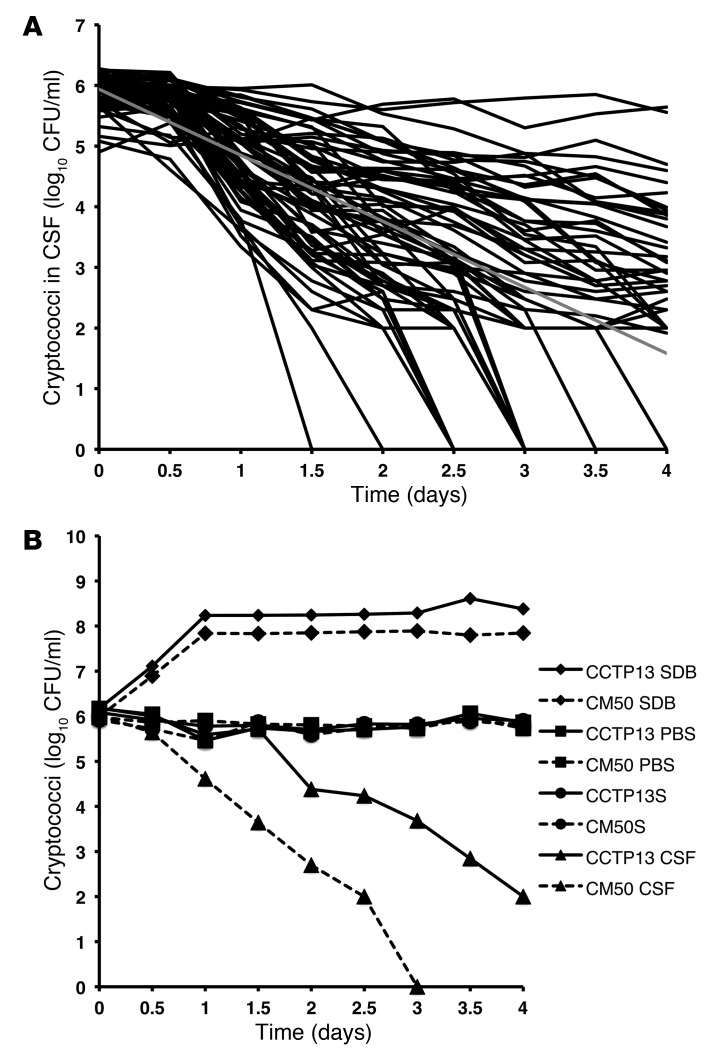
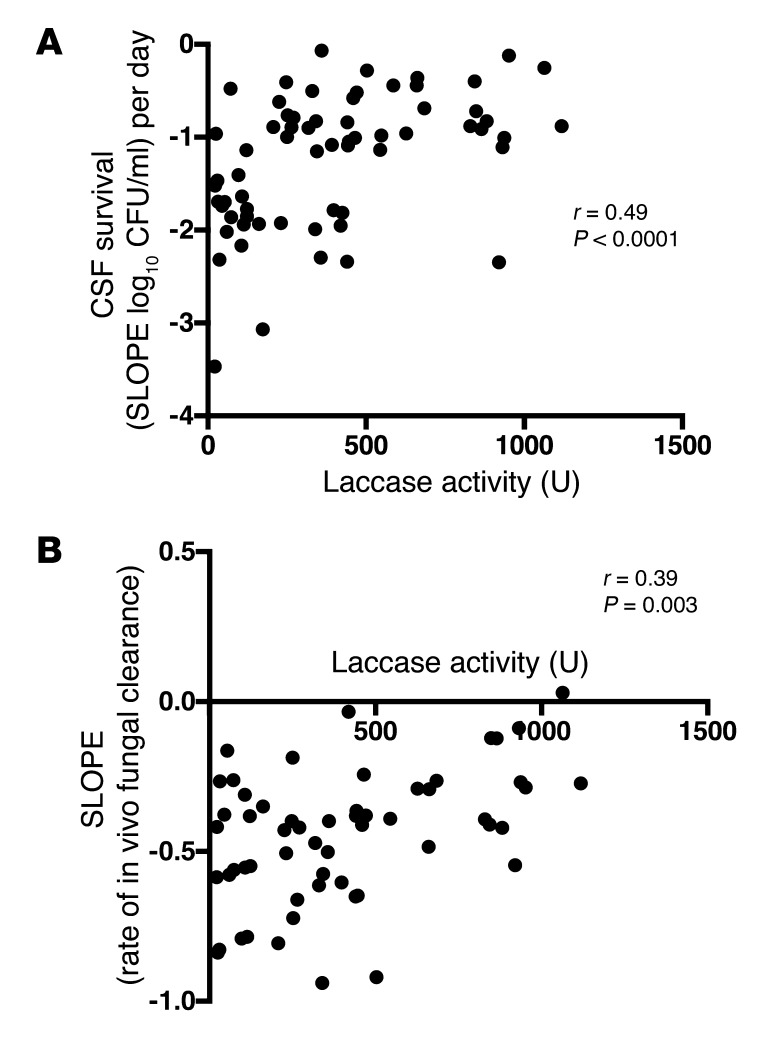
Results: High levels of fungal uptake by macrophages in vitro, but not the IPR, were associated with CSF fungal burden (r = 0.38, P = 0.002) and long-term patient survival (hazard ratio [HR] 2.6, 95% CI 1.2-5.5, P = 0.012). High-uptake strains were hypocapsular (r = -0.28, P = 0.05) and exhibited enhanced laccase activity (r = 0.36, P = 0.003). Fungal isolates with greater laccase activity exhibited heightened survival ex vivo in purified CSF (r = 0.49, P < 0.0001) and resistance to clearance following patient antifungal treatment (r = 0.39, P = 0.003).
Conclusion: These findings underscore the contribution of cryptococcal-phagocyte interactions and laccase-dependent melanin pathways to human clinical presentation and outcome. Furthermore, characterization of fungal-specific pathways that drive clinical manifestation provide potential targets for the development of therapeutics and the management of CM.
Funding: This work was made possible by funding from the Wellcome Trust (WT088148MF), the Medical Research Council (MR/J008176/1), the NIHR Surgical Reconstruction and Microbiology Research Centre and the Lister Institute for Preventive Medicine (to R.C. May), and a Wellcome Trust Intermediate fellowship (089966, to T. Bicanic). The C. neoformans isolates were collected within clinical trials funded by the British Infection Society (fellowship to T. Bicanic), the Wellcome Trust (research training fellowships WT069991, to A.E. Brouwer and WT081794, to J.N. Jarvis), and the Medical Research Council, United Kingdom (76201). The funding sources had no role in the design or conduct of this study, nor in preparation of the manuscript.
Figures
Comment in
-
Cryptococcosis: a model for the understanding of infectious diseases.J Clin Invest. 2014 May;124(5):1893-5. doi: 10.1172/JCI75241. Epub 2014 Apr 17. J Clin Invest. 2014. PMID: 24743152 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
