

Affinity proteomics reveals elevated muscle proteins in plasma of children with cerebral malaria
- PMID: 24743550
- PMCID: PMC3990714
- DOI: 10.1371/journal.ppat.1004038
Affinity proteomics reveals elevated muscle proteins in plasma of children with cerebral malaria
Abstract
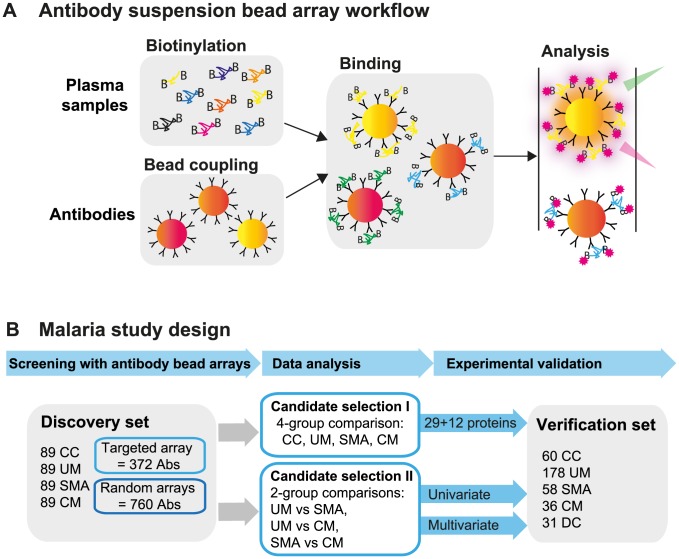
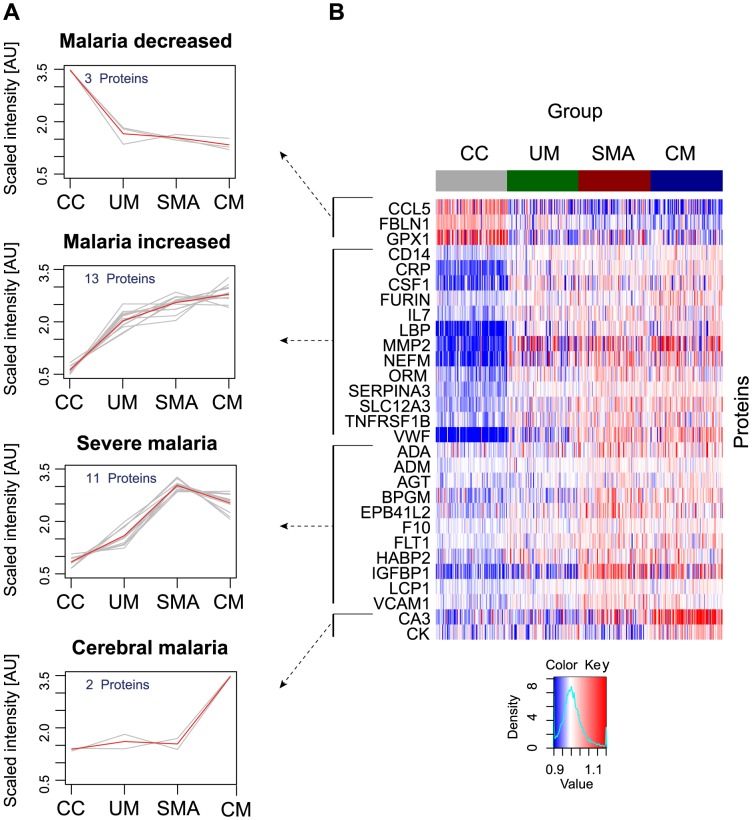
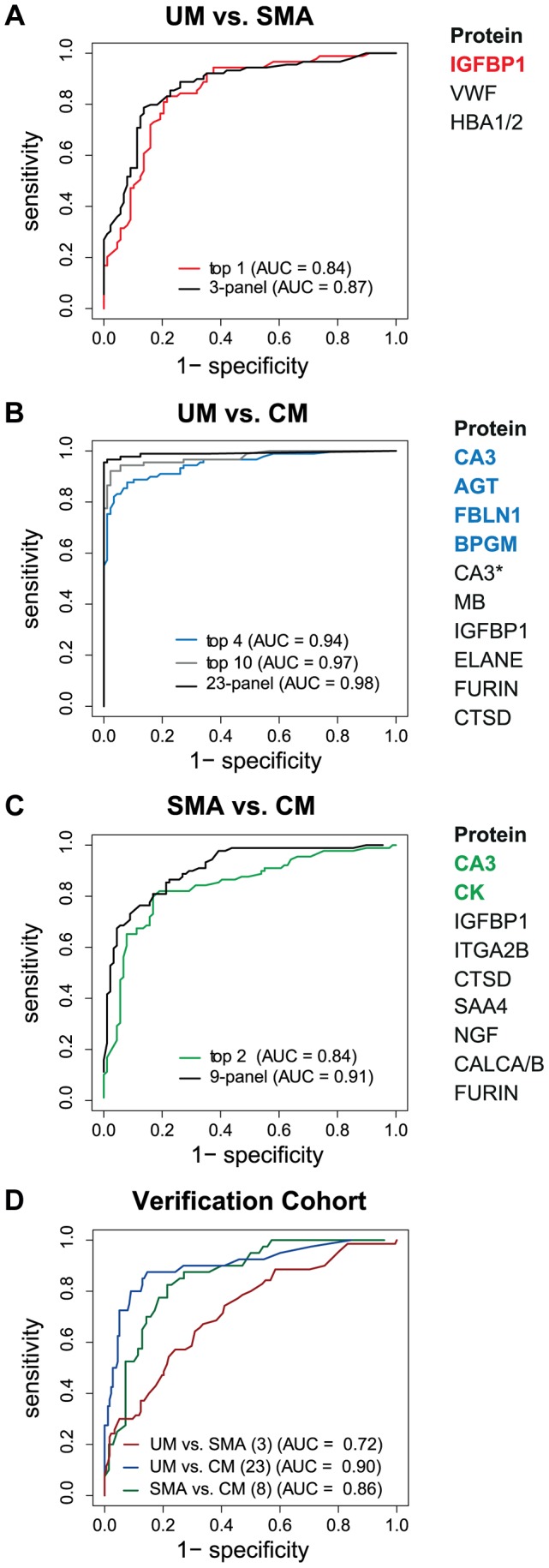
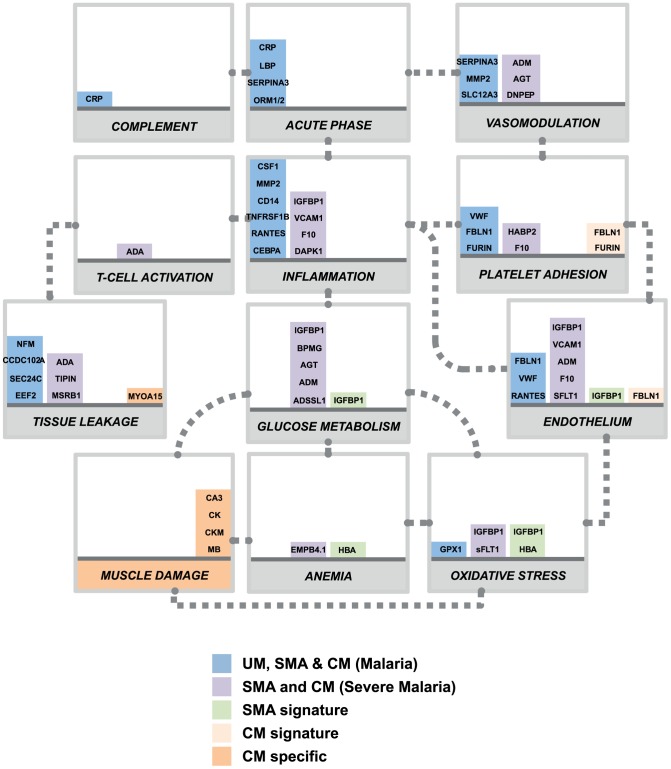
Systemic inflammation and sequestration of parasitized erythrocytes are central processes in the pathophysiology of severe Plasmodium falciparum childhood malaria. However, it is still not understood why some children are more at risks to develop malaria complications than others. To identify human proteins in plasma related to childhood malaria syndromes, multiplex antibody suspension bead arrays were employed. Out of the 1,015 proteins analyzed in plasma from more than 700 children, 41 differed between malaria infected children and community controls, whereas 13 discriminated uncomplicated malaria from severe malaria syndromes. Markers of oxidative stress were found related to severe malaria anemia while markers of endothelial activation, platelet adhesion and muscular damage were identified in relation to children with cerebral malaria. These findings suggest the presence of generalized vascular inflammation, vascular wall modulations, activation of endothelium and unbalanced glucose metabolism in severe malaria. The increased levels of specific muscle proteins in plasma implicate potential muscle damage and microvasculature lesions during the course of cerebral malaria.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization (WHO). (2010). World Malaria Report 2010. Available: http://www.who.int/malaria/world_malaria_report_2010/en/. Last accessed 5th Mar 2014.
-
- Amzat J (2011) Assessing the progress of malaria control in Nigeria. World Health Popul 12: 42–51. - PubMed
-
- Nussler A, Pied S, Pontet M, Miltgen F, Renia L, et al. (1991) Inflammatory status and preerythrocytic stages of malaria: role of the C-reactive protein. Exp Parasitol 72: 1–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
