

Late recurrence of myopic foveoschisis after successful repair with primary vitrectomy and incomplete membrane peeling
- PMID: 24743643
- PMCID: PMC4145023
- DOI: 10.1097/IAE.0000000000000156
Late recurrence of myopic foveoschisis after successful repair with primary vitrectomy and incomplete membrane peeling
Abstract
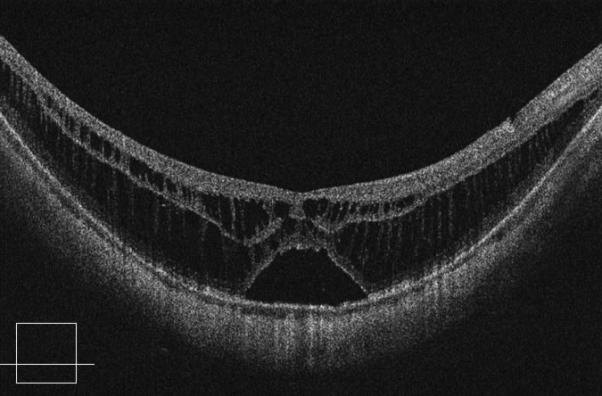
Purpose: To report three cases of late recurrence of myopic foveoschisis (MF) after initial successful repair with pars plana vitrectomy and membrane peeling to assess the importance of internal limiting membrane peeling.
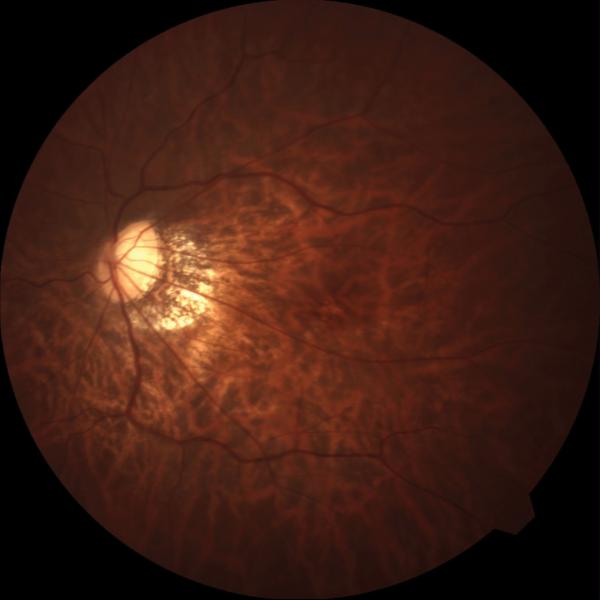
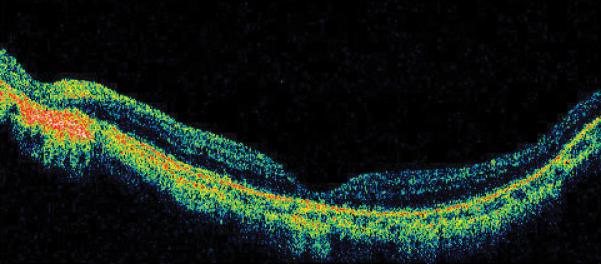
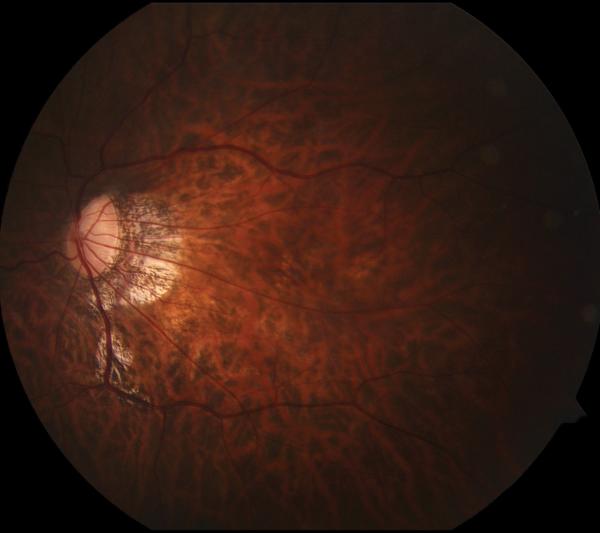
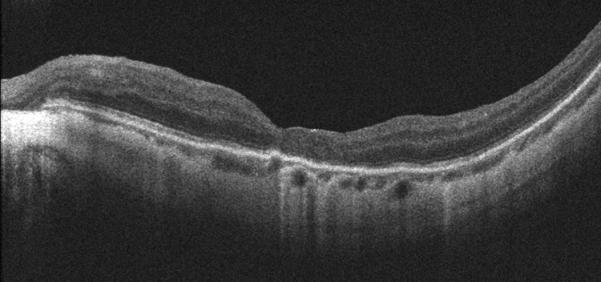
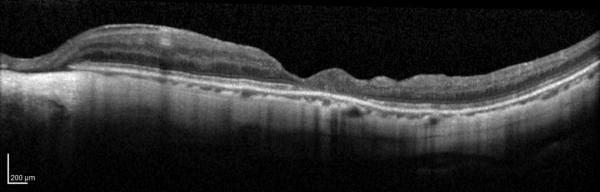
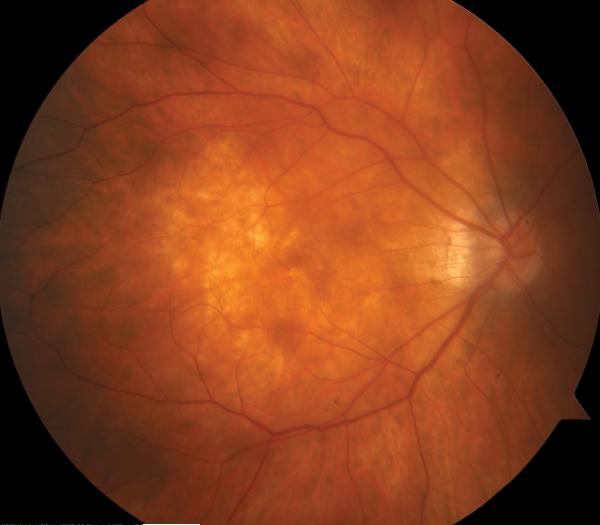
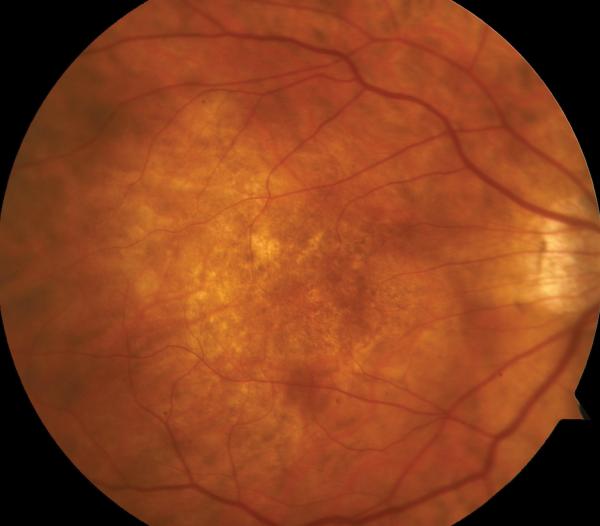
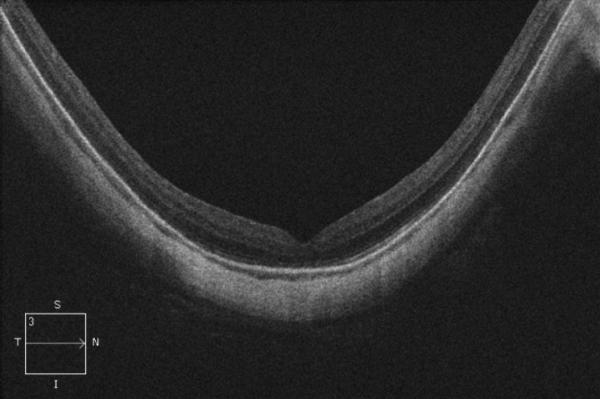
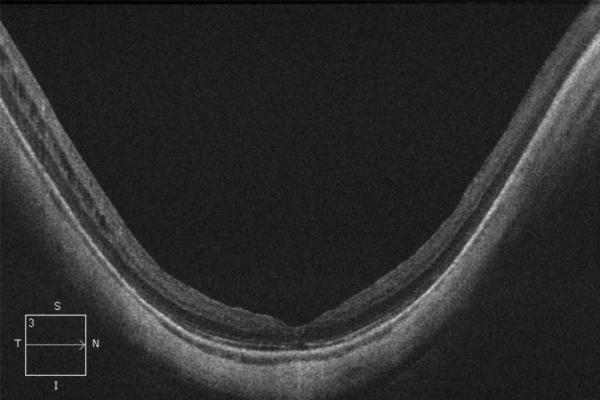
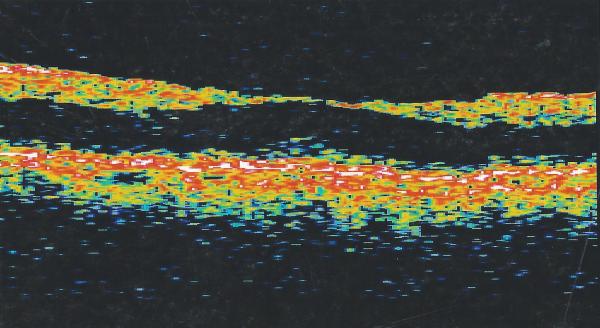
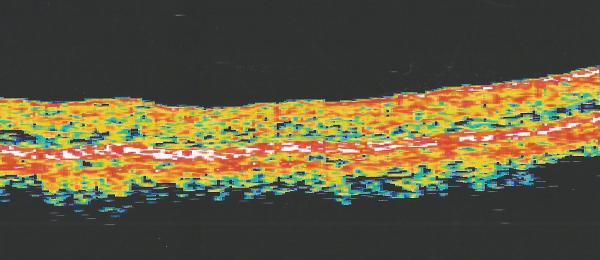
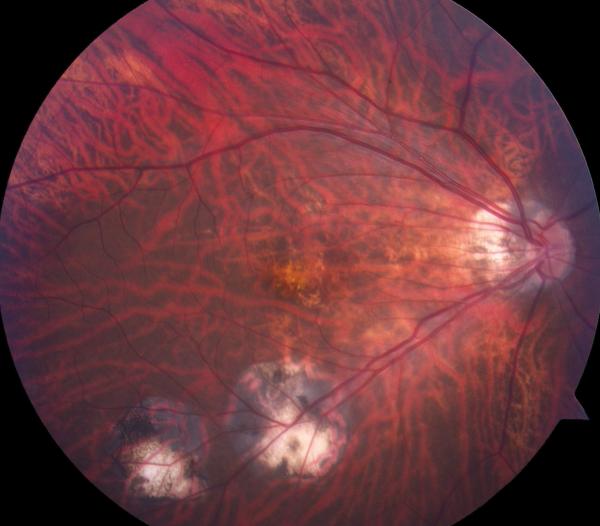
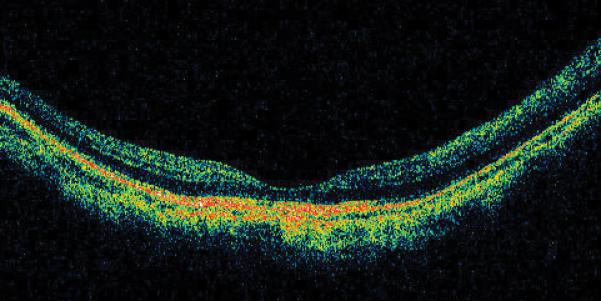
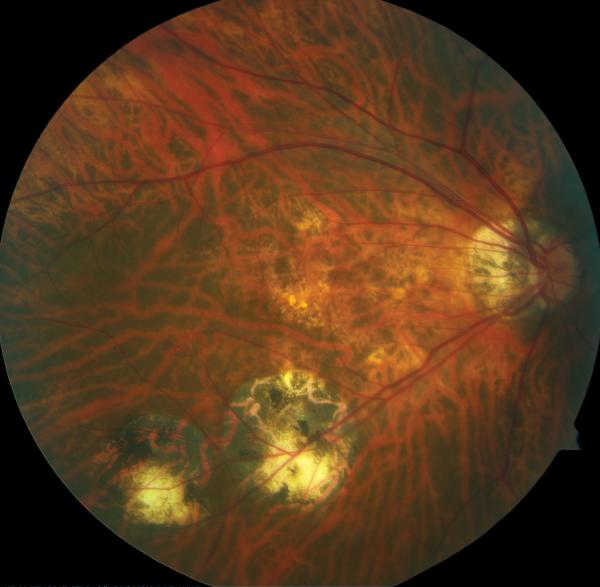
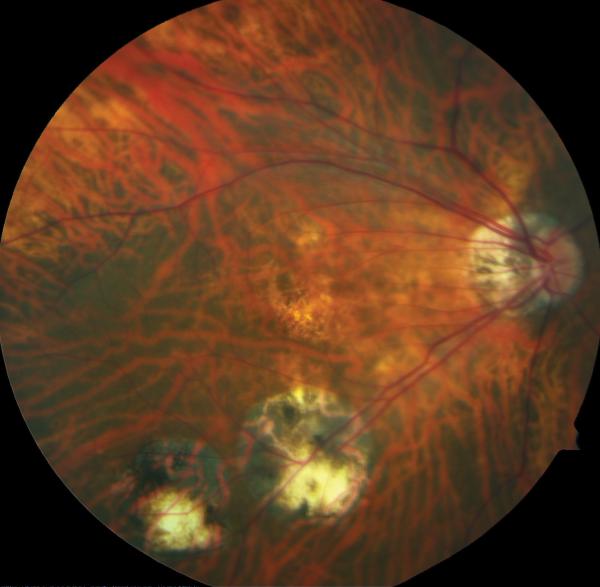
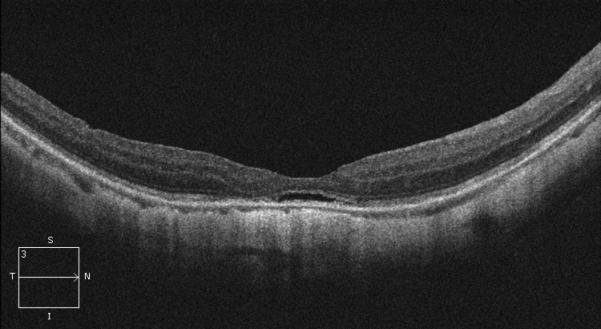
Methods: A retrospective noncomparative case series was performed of patients who underwent a primary pars plana vitrectomy by a single surgeon with successful resolution of MF, but eventually underwent repeat pars plana vitrectomy for recurrent MF. Best-corrected visual acuity, fundus photography, and optical coherence tomography were obtained at each examination.
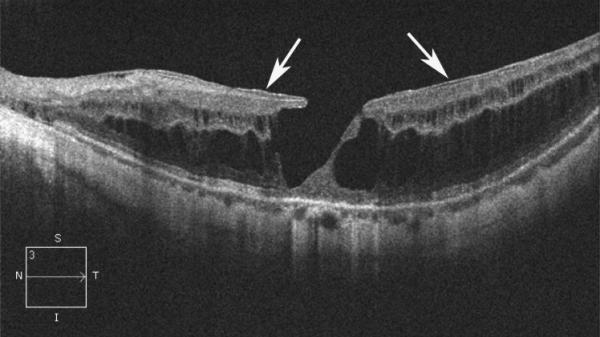
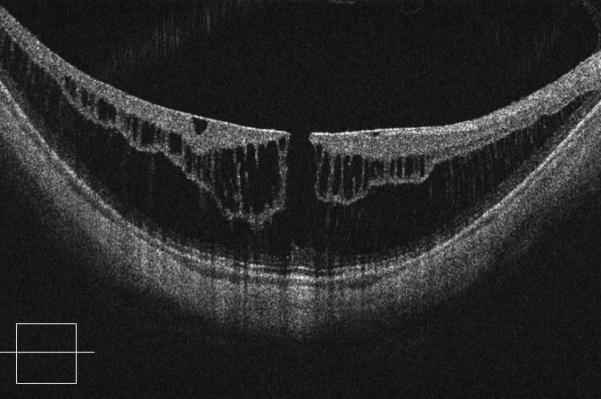
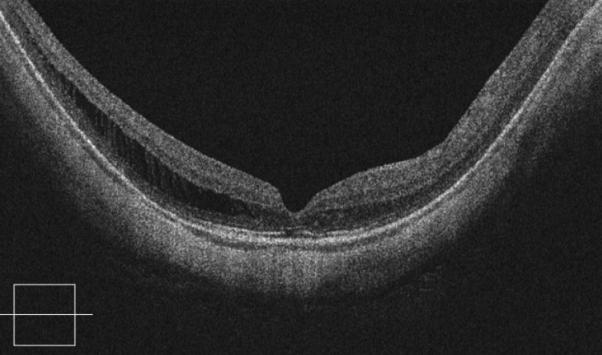
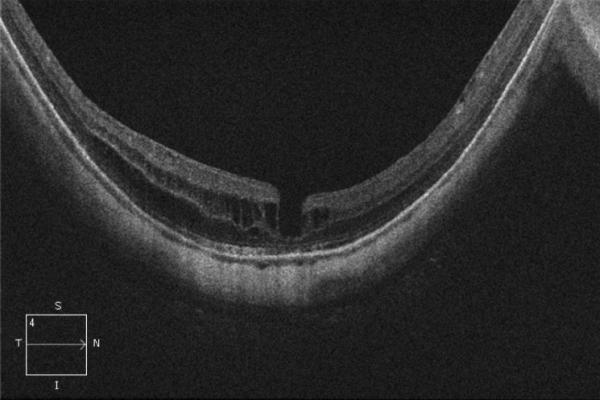
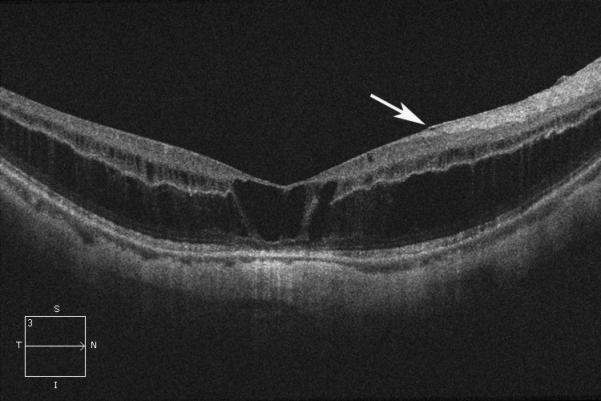
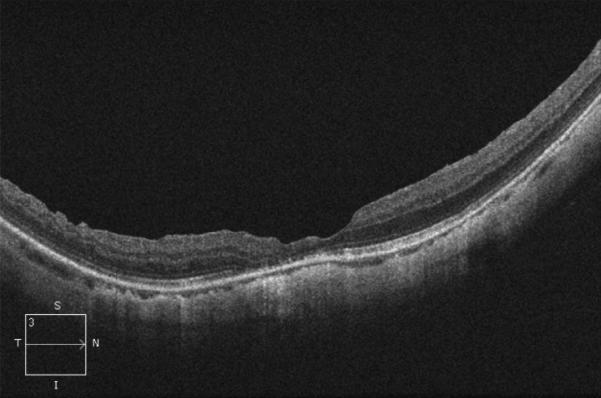
Results: Three eyes of three patients underwent pars plana vitrectomy for recurrent MF. Myopic foveoschisis recurrence occurred 6, 3.5, and 12 years after the primary vitrectomy, respectively. Repeat vitrectomy with staining and additional peeling of the internal limiting membrane resulted in good anatomical outcome and stabilization of visual acuity in all cases.
Conclusion: Late recurrence of MF after successful primary vitrectomy is described. Fibrocellular proliferation on residual cortical vitreous or incomplete internal limiting membrane peeling during the initial vitrectomy may underlie recurrence.
Figures


References
-
- Takano M, Kishi S. Foveal retinoschisis and retinal detachment in severely myopic eyes with posterior staphyloma. Am J Ophthalmol. 1999;128:472–476. - PubMed
-
- Baba T, Ohno-Matsui K, Futagami S, et al. Prevalence and characteristics of foveal retinal detachment without macular hole in high myopia. Am J Ophthalmol. 2003;135:338–342. - PubMed
-
- Gaucher D, Haouchine B, Tadayoni R, et al. Long-term follow-up of high myopic foveoschisis: natural course and surgical outcome. Am J Ophthalmol. 2007;143:455–462. - PubMed
-
- Wu PC, Chen YJ, Chen YH, et al. Factors associated with foveoschisis and foveal detachment without macular hole in high myopia. Eye. 2009;23:356–361. - PubMed
-
- Panozzo G, Mercanti A. Optical coherence tomography findings in myopic traction maculopathy. Arch Ophthalmol. 2004;122:1455–1460. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
