

Beyond race and place: distal sociological determinants of HIV disparities
- PMID: 24743728
- PMCID: PMC3990614
- DOI: 10.1371/journal.pone.0091711
Beyond race and place: distal sociological determinants of HIV disparities
Abstract
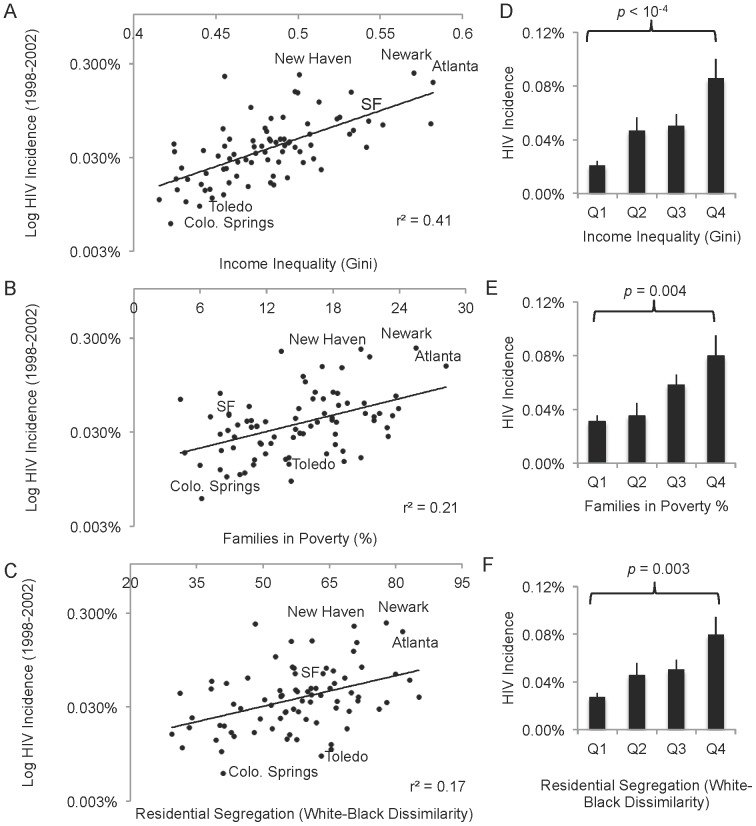
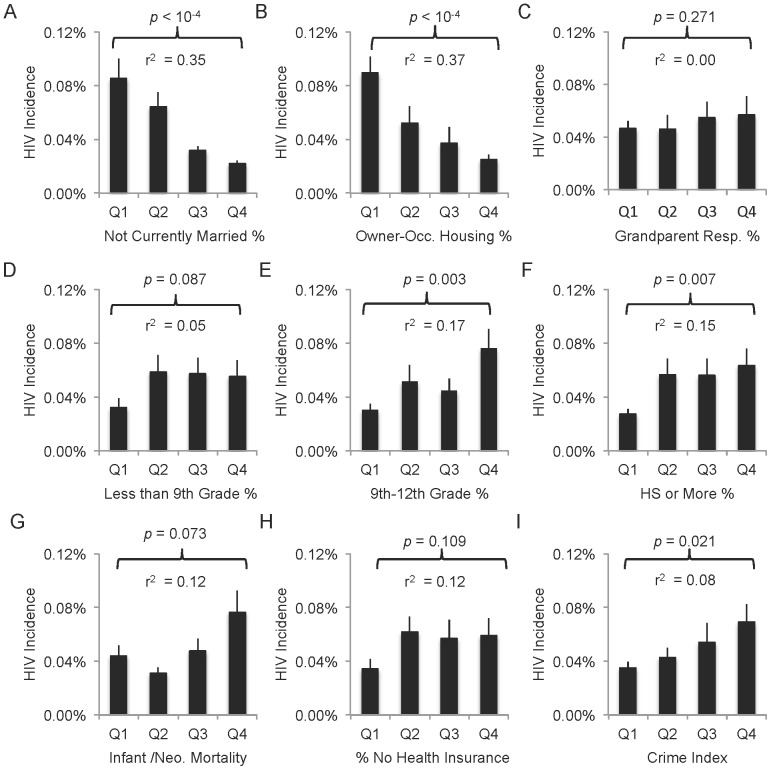
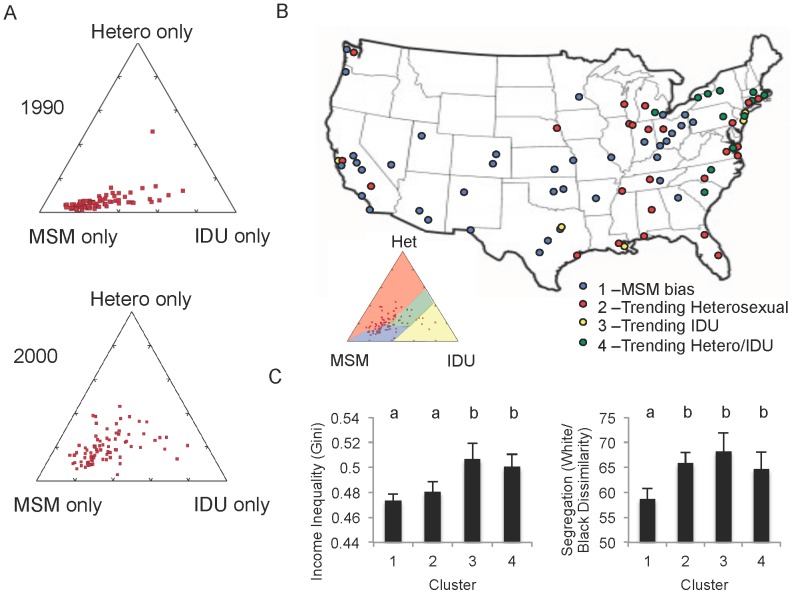
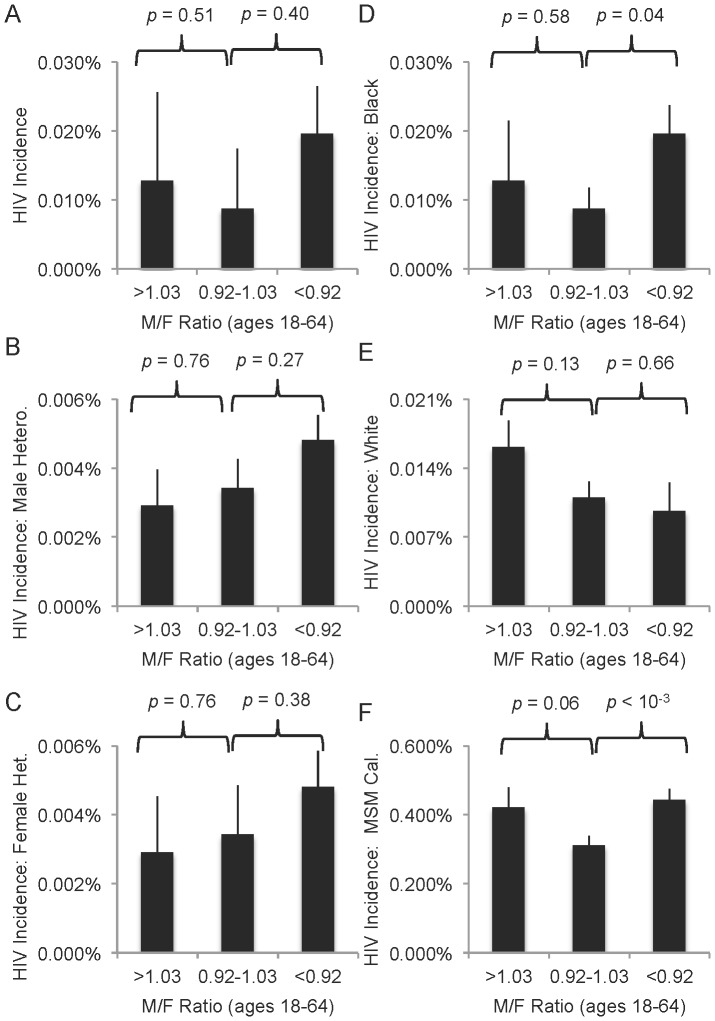
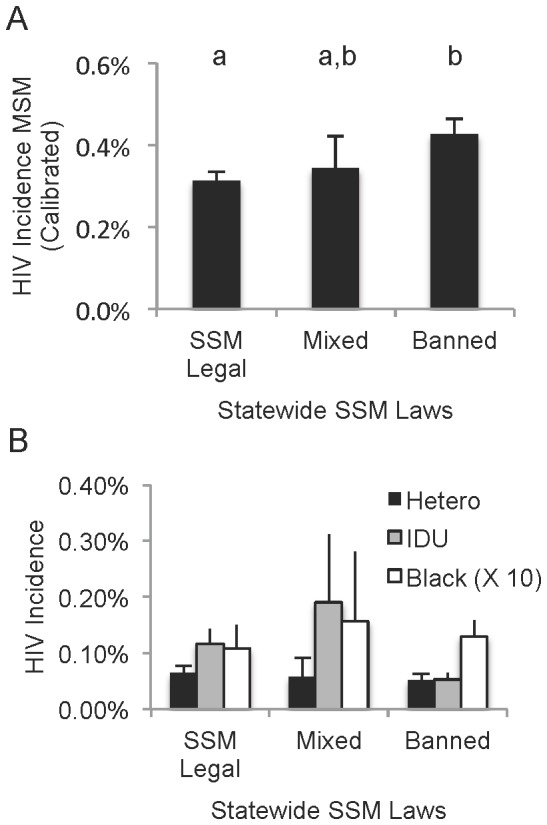
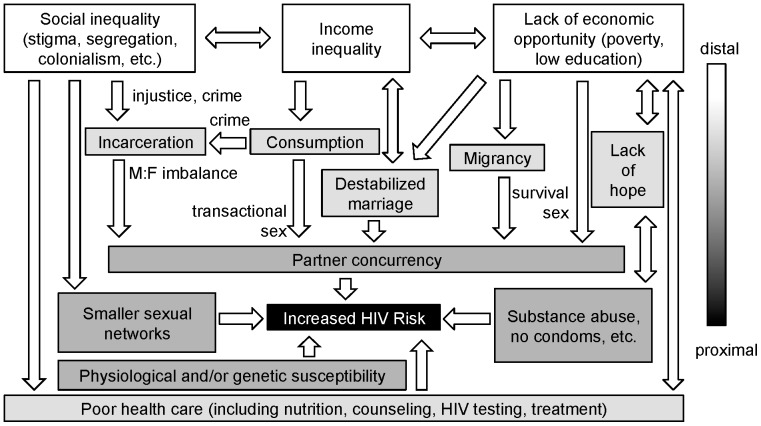
Informed behavior change as an HIV prevention tool has yielded unequal successes across populations. Despite decades of HIV education, some individuals remain at high risk. The mainstream media often portrays these risk factors as products of race and national borders; however, a rich body of recent literature proposes a host of complex social factors that influence behavior, including, but not limited to: poverty, income inequality, stigmatizing social institutions and health care access. We examined the relationship between numerous social indicators and HIV incidence across eighty large U.S. cities in 1990 and 2000. During this time, major correlating factors included income inequality, poverty, educational attainment, residential segregation and marriage rates. However, these ecological factors were weighted differentially across risk groups (e.g. heterosexual, intravenous drug use, men who have sex with men (MSM)). Heterosexual risk rose significantly with poor economic indicators, while MSM risk depended more heavily on anti-homosexual stigma (as measured by same-sex marriage laws). HIV incidence among black individuals correlated significantly with numerous economic factors but also with segregation and imbalances in the male:female ratio (often an effect of mass incarceration). Our results support an overall model of HIV ecology where poverty, income inequality and social inequality (in the form of institutionalized racism and anti-homosexual stigma) have over time developed into synergistic drivers of disease transmission in the U.S., inhibiting information-based prevention efforts. The relative weights of these distal factors vary over time and by HIV risk group. Our testable model may be more generally applicable within the U.S. and beyond.
Conflict of interest statement
Figures
References
-
- UNAIDS (2007) Practical guidelines for intensifying HIV prevention: towards universal access. In: HIV/AIDS. JUNPo, editor. Geneva: UNAIDS.
-
- Centers for Disease Control and Prevention (2013) HIV/AIDS Surveillance Report Vol. 23.
-
- Mosher WD, Chandra A, Jones J (2005) Sexual behavior and selected health measures: men and women 15–44 years of age, United States, 2002. Advance data 1–55. - PubMed
-
- Harawa NT, Greenland S, Cochran SD, Cunningham WE, Visscher B (2003) Do differences in relationship and partner attributes explain disparities in sexually transmitted disease among young white and black women? The Journal of adolescent health : official publication of the Society for Adolescent Medicine 32: 187–191. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
