

Developing a new electromyography-based algorithm to diagnose the etiology of fecal incontinence
- PMID: 24743845
- PMCID: PMC4028542
- DOI: 10.1007/s00384-014-1859-1
Developing a new electromyography-based algorithm to diagnose the etiology of fecal incontinence
Abstract
Purpose: For surface electromyography (sEMG) to become widely used in fecal incontinence (FI) etiology assessment, one would have to create a simple, step-by-step, computer-aided, electromyography-based algorithm that would become the basis for a computer-aided diagnosis (CAD) system. Thus, the aim of this work was to develop such an algorithm.
Methods: Each patient included in the study underwent a structured medical interview, a general physical examination, and a proctological examination. Patients that scored more than 10 points on the fecal incontinence severity index (FISI) underwent further tests that included rectoscopy, anorectal manometry, transanal ultrasonography, multichannel sEMG, and assessment of anal reflexes. Patients with fully diagnosed FI were included into the study group. The control group consisted of healthy volunteers that scored five or less points on the FISI and had no known anal sphincters dysfunction.
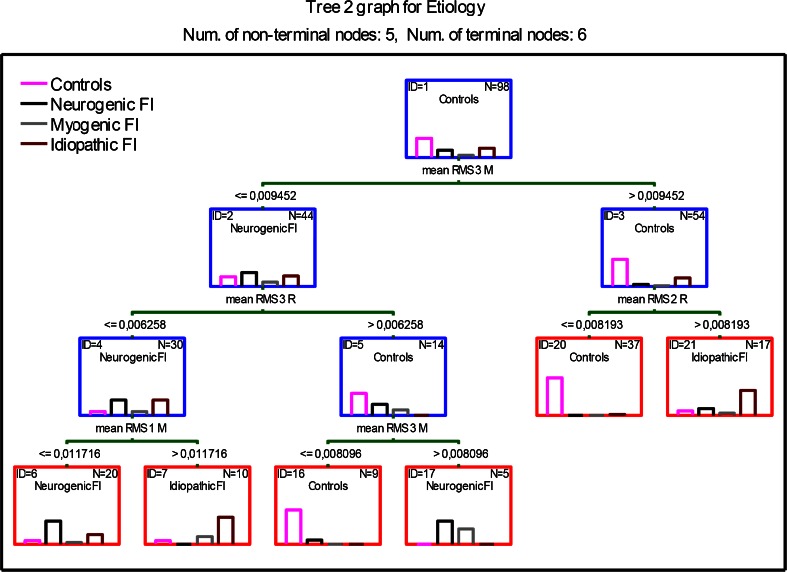
Results: Forty-nine patients were qualified to the study group (age ± SD 58.9 ± 13.8). The control group was number- and gender-matched (age ± SD 45.4 ± 15.1). The sensitivity and specificity of classification tree number I, to diagnose neurogenic FI, were 89.5 and 86 %, respectively. For patients with idiopathic FI, these values were 82 and 91 %, respectively. The sensitivity and specificity of classification tree number III, to diagnose neurogenic FI, were 84 and 78 %, respectively. For patients with idiopathic FI, these values were 78 and 87 %, respectively.
Conclusions: The relative simplicity and low classification costs allow to assume that algorithms based on classification trees I and III will serve to be the basis for a FI etiology CAD system.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
