

Surgical revascularization is associated with maximal survival in patients with ischemic mitral regurgitation: a 20-year experience
- PMID: 24744275
- PMCID: PMC4142433
- DOI: 10.1161/CIRCULATIONAHA.113.005223
Surgical revascularization is associated with maximal survival in patients with ischemic mitral regurgitation: a 20-year experience
Abstract
Background: The optimal treatment for ischemic mitral regurgitation remains actively debated. Our objective was to evaluate the relationship between ischemic mitral regurgitation treatment strategy and survival.
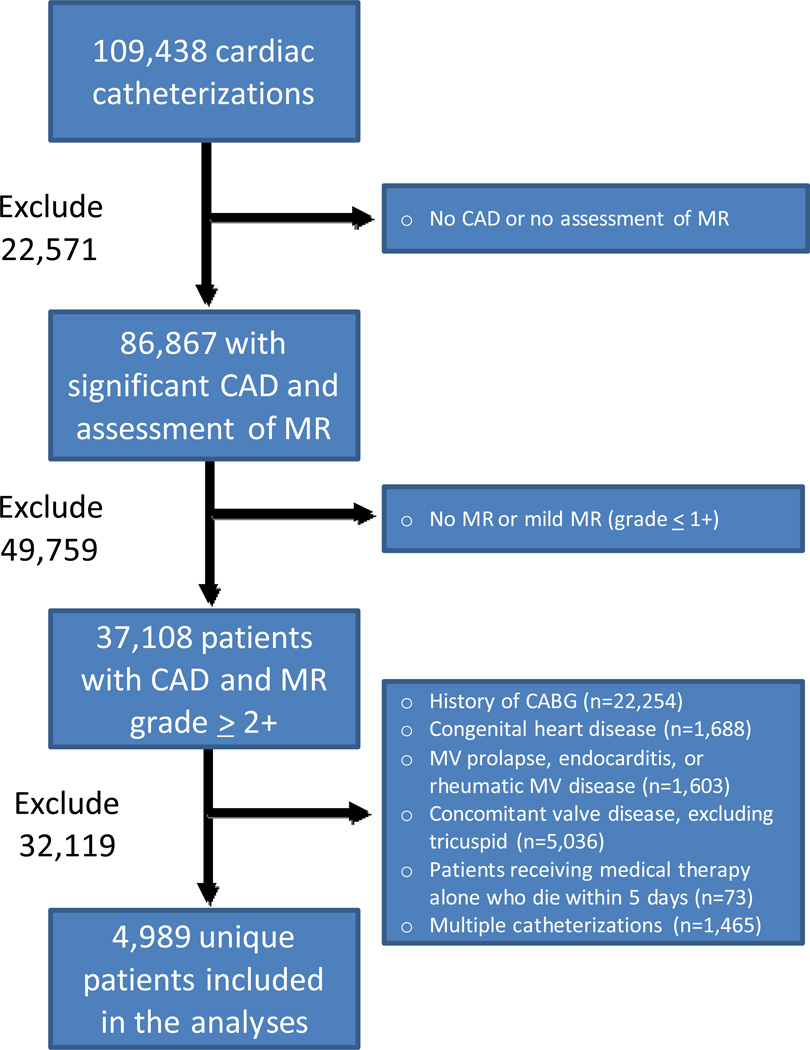
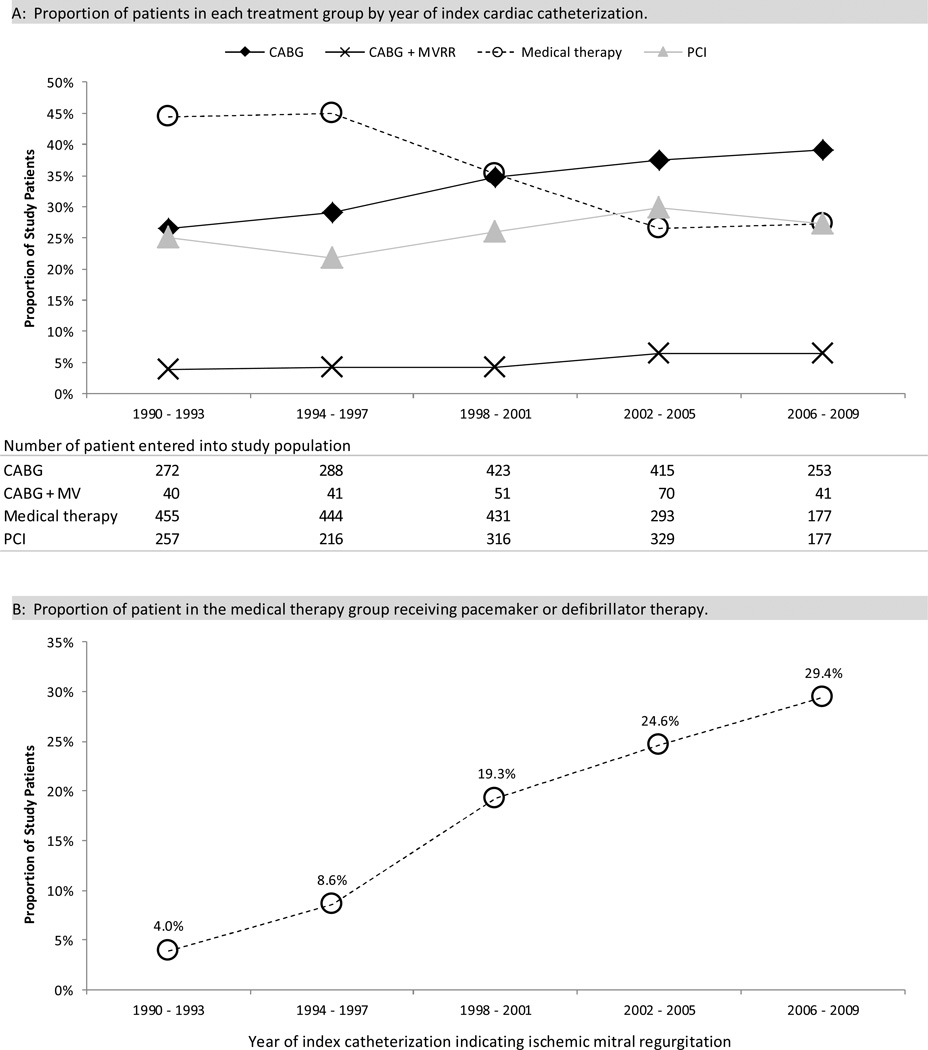
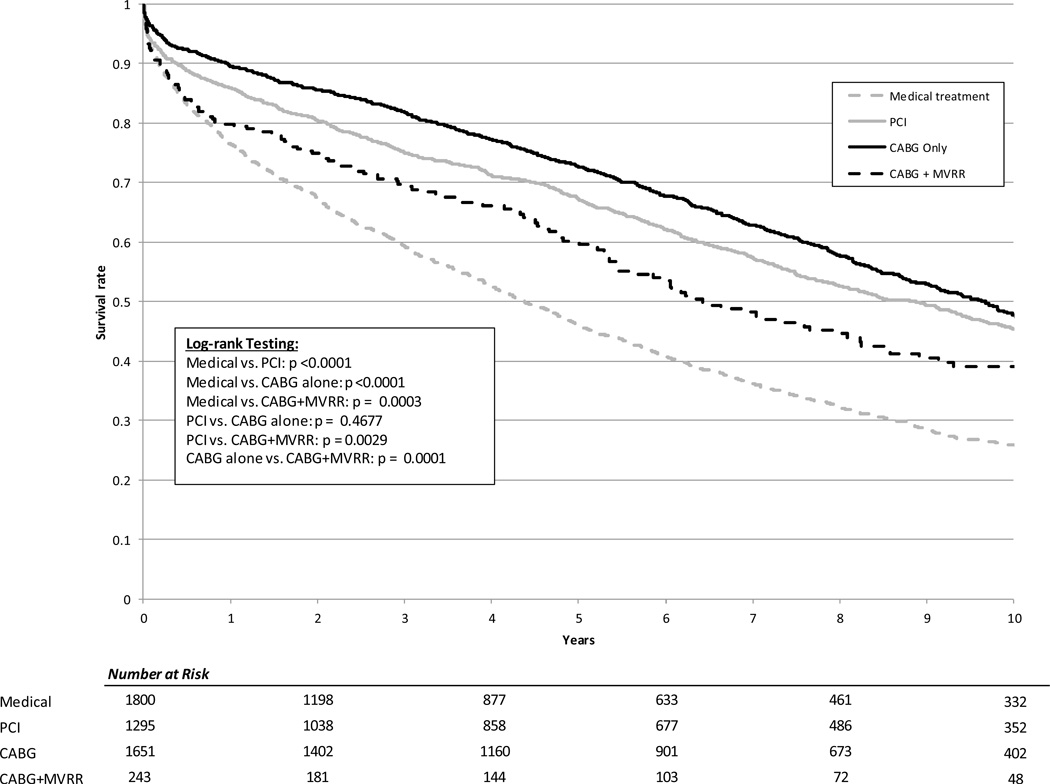
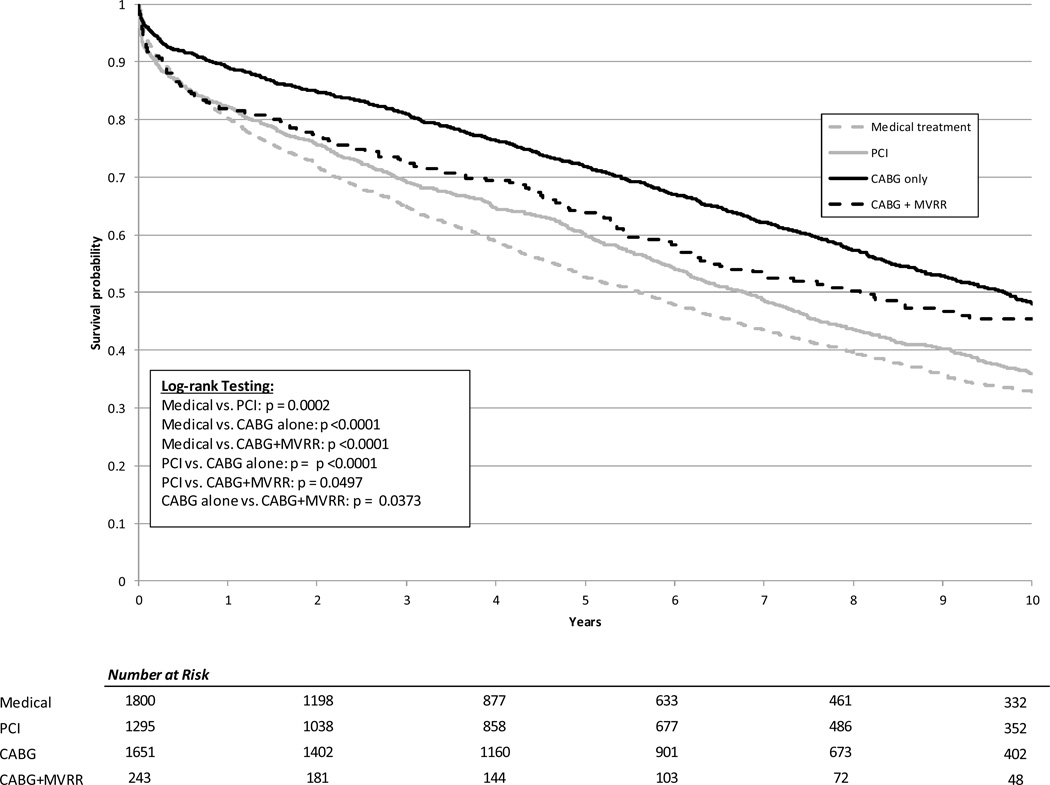
Methods and results: We retrospectively reviewed patients at our institution diagnosed with significant coronary artery disease and moderate or severe ischemic mitral regurgitation from 1990 to 2009, categorized by medical treatment alone, percutaneous coronary intervention, coronary artery bypass grafting (CABG), or CABG plus mitral valve repair or replacement. Kaplan-Meier methods and multivariable Cox proportional hazards analyses were performed to assess the relationship between treatment strategy and survival, with the use of propensity scores to account for nonrandom treatment assignment. A total of 4989 patients were included: medical treatment alone=36%, percutaneous coronary intervention=26%, CABG=33%, and CABG plus mitral valve repair or replacement=5%. Median follow-up was 5.37 years. Compared with medical treatment alone, significantly lower mortality was observed in patients treated with percutaneous coronary intervention (adjusted hazard ratio, 0.83; 95% confidence interval, 0.76-0.92; P=0.0002), CABG (adjusted hazard ratio, 0.56; 95% confidence interval, 0.51-0.62; P<0.0001), and CABG plus mitral valve repair or replacement (adjusted hazard ratio, 0.69; 95% confidence interval, 0.57-0.82; P<0.0001). There was no significant difference in these results based on mitral regurgitation severity.
Conclusions: Patients with significant coronary artery disease and moderate or severe ischemic mitral regurgitation undergoing CABG alone demonstrated the lowest risk of death. CABG with or without mitral valve surgery was associated with lower mortality than either percutaneous coronary intervention or medical treatment alone.
Keywords: ischemia; mitral valve; revascularization; stent.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Figures
Comment in
-
Letter by Durukan regarding article, "surgical revascularization is associated with maximal survival in patients with ischemic mitral regurgitation: a 20-year experience".Circulation. 2015 Mar 17;131(11):e377. doi: 10.1161/CIRCULATIONAHA.114.010940. Circulation. 2015. PMID: 25779549 No abstract available.
-
Response to letter regarding article, "surgical revascularization is associated with maximal survival in patients with ischemic mitral regurgitation: a 20-year experience".Circulation. 2015 Mar 17;131(11):e378-9. doi: 10.1161/CIRCULATIONAHA.114.013125. Circulation. 2015. PMID: 25779550 Free PMC article. No abstract available.
Similar articles
-
Coronary revascularization alone or with mitral valve repair: outcomes in patients with moderate ischemic mitral regurgitation.Tex Heart Inst J. 2009;36(5):416-24. Tex Heart Inst J. 2009. PMID: 19876417 Free PMC article.
-
Survival after coronary revascularization, with and without mitral valve surgery, in patients with ischemic mitral regurgitation.Circulation. 2003 Sep 9;108 Suppl 1:II103-10. doi: 10.1161/01.cir.0000087656.10829.df. Circulation. 2003. PMID: 12970217
-
Mitral regurgitation surgery in patients with ischemic cardiomyopathy and ischemic mitral regurgitation: factors that influence survival.J Thorac Cardiovasc Surg. 2011 Nov;142(5):995-1001. doi: 10.1016/j.jtcvs.2011.07.044. Epub 2011 Aug 19. J Thorac Cardiovasc Surg. 2011. PMID: 21855899
-
Does combined mitral valve surgery improve survival when compared to revascularization alone in patients with ischemic mitral regurgitation? A meta-analysis on 2479 patients.J Cardiovasc Med (Hagerstown). 2009 Feb;10(2):109-14. doi: 10.2459/JCM.0b013e32831c84b0. J Cardiovasc Med (Hagerstown). 2009. PMID: 19377377 Review.
-
Mitral valve surgery and coronary artery bypass grafting for moderate-to-severe ischemic mitral regurgitation: Meta-analysis of clinical and echocardiographic outcomes.J Thorac Cardiovasc Surg. 2017 Jul;154(1):127-136. doi: 10.1016/j.jtcvs.2017.03.039. Epub 2017 Mar 22. J Thorac Cardiovasc Surg. 2017. PMID: 28549693
Cited by
-
OPCABG for Moderate CIMR in Elderly Patients: a Superior Option?Braz J Cardiovasc Surg. 2018 Jan-Feb;33(1):15-22. doi: 10.21470/1678-9741-2017-0114. Braz J Cardiovasc Surg. 2018. PMID: 29617497 Free PMC article.
-
Baseline mitral regurgitation predicts outcome in patients referred for dobutamine stress echocardiography.Int J Cardiovasc Imaging. 2017 Nov;33(11):1711-1721. doi: 10.1007/s10554-017-1163-6. Epub 2017 Jul 6. Int J Cardiovasc Imaging. 2017. PMID: 28685313 Free PMC article.
-
Surgical Treatment of Ischemic Mitral Regurgitation: Valve Repair Versus Replacement.Curr Cardiol Rep. 2017 Jan;19(1):3. doi: 10.1007/s11886-017-0813-6. Curr Cardiol Rep. 2017. PMID: 28101839 Review.
-
Best treatment option for secondary mitral regurgitation surgery: a network meta-analysis of randomized and non-randomized controlled studies.Sci Rep. 2024 Oct 14;14(1):24037. doi: 10.1038/s41598-024-75173-y. Sci Rep. 2024. PMID: 39402122 Free PMC article.
-
Prosthetic Mitral Valve Thrombosis: A Complication Following Mitral Valve Surgery and Coronary Artery Bypass Graft Surgery.Cureus. 2022 Aug 14;14(8):e28013. doi: 10.7759/cureus.28013. eCollection 2022 Aug. Cureus. 2022. PMID: 36134064 Free PMC article.
References
-
- HCUPnet. Healthcare Cost and Utilization Project (HCUP) Rockville, MD: Agency for Healthcare Research and Quality; 2010. [Accessed July 15, 2012]. http://hcupnet.ahrq.gov/ - PubMed
-
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, Ford E, Furie K, Go A, Greenlund K, Haase N, Hailpern S, Ho M, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott M, Meigs J, Mozaffarian D, Nichol G, O'Donnell C, Roger V, Rosamond W, Sacco R, Sorlie P, Stafford R, Steinberger J, Thom T, Wasserthiel-Smoller S, Wong N, Wylie-Rosett J, Hong Y. Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:e21–e181. - PubMed
-
- Birnbaum Y, Chamoun AJ, Conti VR, Uretsky BF. Mitral regurgitation following acute myocardial infarction. Coron Artery Dis. 2002;13:337–344. - PubMed
-
- Bursi F, Enriquez-Sarano M, Jacobsen SJ, Roger VL. Mitral regurgitation after myocardial infarction: a review. Am J Med. 2006;119:103–112. - PubMed
-
- Carabello BA. The current therapy for mitral regurgitation. J Am Coll Cardiol. 2008;52:319–326. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
