Pharmacology of the lower urinary tract
- PMID: 24744518
- PMCID: PMC3989821
- DOI: 10.4103/0970-1591.126903
Pharmacology of the lower urinary tract
Abstract
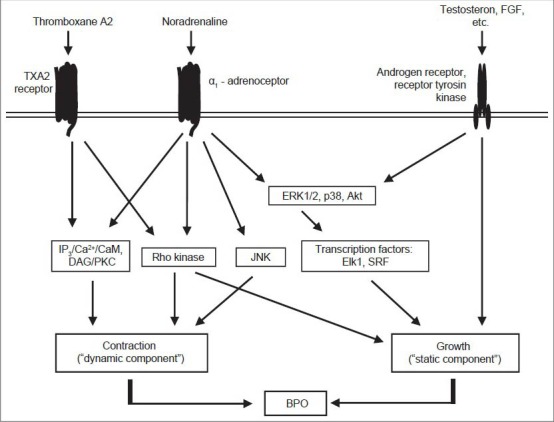
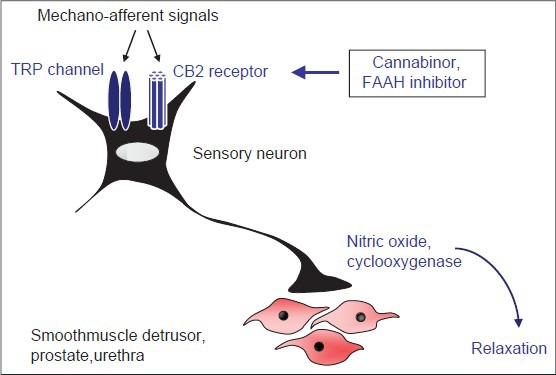
Pharmacology of the lower urinary tract provides the basis for medical treatment of lower urinary tract symptoms (LUTS). Therapy of LUTS addresses obstructive symptoms (frequently explained by increased prostate smooth muscle tone and prostate enlargement) in patients with benign prostate hyperplasia (BPH) and storage symptoms in patients with overactive bladder (OAB). Targets for medical treatment include G protein-coupled receptors (α1-adrenoceptors, muscarinic acetylcholine receptors, β3-adrenoceptors) or intracellular enzymes (5α-reductase; phosphodiesterase-5, PDE5). Established therapies of obstructive symptoms aim to induce prostate smooth muscle relaxation by α1-blockers or PDE5 inhibitors, or to reduce prostate growth and volume with 5α-reductase inhibitors. Available options for treatment of OAB comprise anitmuscarinics, β3-adrenoceptor agonists, and botulinum toxin A, which improve storage symptoms by inhibition of bladder smooth muscle contraction. With the recent approval of β3-antagonists, PDE inhibitors, and silodosin for therapy of LUTS, progress from basic research of lower urinary tract pharmacology was translated into new clinical applications. Further targets are in preclinical stages of examination, including modulators of the endocannabinoid system and transient receptor potential (TRP) channels.
Keywords: 5 alpha reductase; Alpha1 adrenoreceptor; arginine vasopressors; endocannabinoids; muscarinic receptors; phosphodiesterase; vitamin D.
Conflict of interest statement
Figures

Similar articles
-
[Benign Prostate Hyperplasia - Current Medical Therapy, New Developments, and Side Effects].Ther Umsch. 2023 Apr;80(3):113-122. doi: 10.1024/0040-5930/a001423. Ther Umsch. 2023. PMID: 36975030 German.
-
Concentration-dependent alpha1-Adrenoceptor Antagonism and Inhibition of Neurogenic Smooth Muscle Contraction by Mirabegron in the Human Prostate.Front Pharmacol. 2021 Jun 24;12:666047. doi: 10.3389/fphar.2021.666047. eCollection 2021. Front Pharmacol. 2021. PMID: 34248624 Free PMC article.
-
Current medical treatment of lower urinary tract symptoms/BPH: do we have a standard?Curr Opin Urol. 2014 Jan;24(1):21-8. doi: 10.1097/MOU.0000000000000007. Curr Opin Urol. 2014. PMID: 24231531 Review.
-
Latest treatment for lower urinary tract dysfunction: therapeutic agents and mechanism of action.Int J Urol. 2013 Jan;20(1):28-39. doi: 10.1111/iju.12008. Epub 2012 Nov 28. Int J Urol. 2013. PMID: 23190275 Review.
-
New therapeutic strategies for the treatment of male lower urinary tract symptoms.Res Rep Urol. 2016 Apr 26;8:51-9. doi: 10.2147/RRU.S63446. eCollection 2016. Res Rep Urol. 2016. PMID: 27218069 Free PMC article. Review.
Cited by
-
An immunohistochemical identification key for cell types in adult mouse prostatic and urethral tissue sections.PLoS One. 2017 Nov 16;12(11):e0188413. doi: 10.1371/journal.pone.0188413. eCollection 2017. PLoS One. 2017. PMID: 29145476 Free PMC article.
-
Possible role of transient receptor potential melastatin 4 channels in adrenergic contractions in mouse prostate smooth muscles.J Vet Med Sci. 2023 Jul 1;85(7):705-714. doi: 10.1292/jvms.23-0112. Epub 2023 May 23. J Vet Med Sci. 2023. PMID: 37225446 Free PMC article.
-
Inhibition of prostate smooth muscle contraction and prostate stromal cell growth by the inhibitors of Rac, NSC23766 and EHT1864.Br J Pharmacol. 2015 Jun;172(11):2905-17. doi: 10.1111/bph.13099. Epub 2015 May 5. Br J Pharmacol. 2015. PMID: 25631101 Free PMC article.
-
Vitamin D deficiency and lower urinary tract symptoms in males above 50 years of age.Urol Ann. 2017 Apr-Jun;9(2):170-173. doi: 10.4103/0974-7796.204192. Urol Ann. 2017. PMID: 28479770 Free PMC article.
-
Re: Efficacy of tadalafil treatment in erectile dysfunction in patients receiving dutasteride treatment: A prospective nonrandomized comparative study.Turk J Urol. 2019 Dec;45(Supp. 1):S192-S193. doi: 10.5152/tud.2019.92604. Epub 2019 Dec 1. Turk J Urol. 2019. PMID: 33120013 Free PMC article. No abstract available.
References
-
- Andersson KE, Lepor H, Wyllie MG. Prostatic alpha 1-adrenoceptors and uroselectivity. Prostate. 1997;30:202–15. - PubMed
-
- Roehrborn CG, Schwinn DA. Alpha1-adrenergic receptors and their inhibitors in lower urinary tract symptoms and benign prostatic hyperplasia. J Urol. 2004;171:1029–35. - PubMed
-
- Madersbacher S, Marszalek M, Lackner J, Berger P, Schatzl G. The long-term outcome of medical therapy for BPH. Eur Urol. 2007;51:1522–33. - PubMed
-
- Andersson KE. Antimuscarinic mechanisms and the overactive detrusor: An update. Eur Urol. 2011;59:377–86. - PubMed
-
- Chapple CR, Wein AJ, Abrams P, Dmochowski RR, Giuliano F, Kaplan SA, et al. Lower urinary tract symptoms revisited: A broader clinical perspective. Eur Urol. 2008;54:563–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources