

Chorea, Hyperglycemia, Basal Ganglia Syndrome (C-H-BG) in an uncontrolled diabetic patient with normal glucose levels on presentation
- PMID: 24744820
- PMCID: PMC3989942
- DOI: 10.12659/AJCR.890179
Chorea, Hyperglycemia, Basal Ganglia Syndrome (C-H-BG) in an uncontrolled diabetic patient with normal glucose levels on presentation
Abstract
Patient: Female, 66 FINAL DIAGNOSIS: Chorea • hyperglycemia • Basal Ganglia Syndrome (C-H-BG) Symptoms: Hemibalism • hemichorea
Medication: - Clinical Procedure: - Specialty: Endocrinology and Metabolic.
Objective: Challenging differential diagnosis.
Background: Hemichorea-hemiballism (HCHB) is a spectrum of involuntary, continuous non-patterned movement involving 1 side of the body. Possible causes of HCHB include hemorrhagic or ischemic stroke, neoplasm, systemic lupus erythematosus, HHNK, Wilson's disease, and thyrotoxicosis. This case illustrates the need to be aware of hyperglycemia as a cause of hemiballism/hemichorea, which is now referred to in the medical literature as C-H-BG (chorea, hyperglycemia, basal ganglia) syndrome.
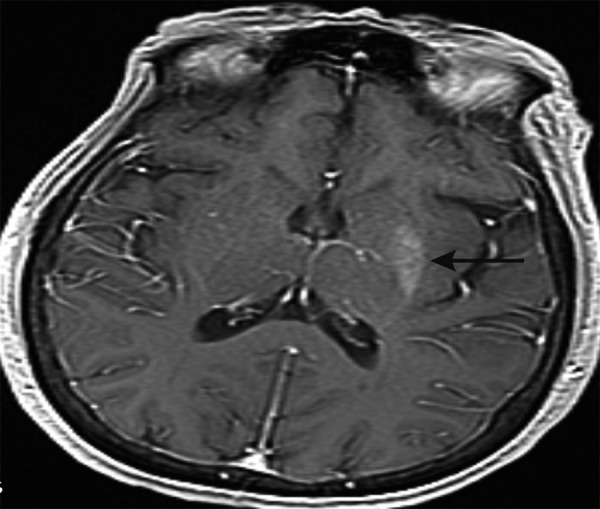
Case report: A 66-year-old Hispanic woman presented to our care with hemiballism/hemichorea of the right arm and leg of 1 week duration. She had been admitted 3 months prior with toxic metabolic encephalopathy secondary to hyperosmolar hyperglycemic non-ketotic syndrome with a blood glucose level of 984 mg/dL. Her blood glucose level was normal but hemoglobin A1C was 12.2%. A brain MRI revealed an asymmetric T1 hyperintensity of the left putamen. This specific finding was compatible with hyperglycemia-induced hemichorea hemiballism syndrome. The hemiballism/hemichorea slowly improved over the course of the hospitalization with strict glycemic control. At the 3-month follow-up visit she had no involuntary movements of her extremities, and she had well controlled blood glucose levels and a hemoglobin A1C of 9.0.
Conclusions: In a patient with normal glycemic levels but a history of uncontrolled diabetes, C-H-BG syndrome should be on the top of the differential list when the characteristic MRI findings of a hyperintensity in the basal ganglia are observed. This is a rare disease that deserves attention because it is reversible with correction of hyperglycemia. Thus, prompt recognition and treatment is essential to avoid adverse outcomes.
Keywords: Basal Ganglia Diseases; Chorea; Dyskinesias; Hyperglycinemia, Nonketotic.
Figures
References
-
- Qi X, Yan Y, Gao Y, Zheng Z, Chang Y. Hemichorea associated with non-ketotic hyperglycaemia: a case report. Diabetes Res Clin Pract. 2012;95(1):e1–e3. - PubMed
-
- Battisi C, Forte F, Rubenni E, et al. Two cases of hemichorea-hemiballism with nonketotic hyperglycemia: a new point of view. Neurol Sci. 2009;30(3):179–83. - PubMed
-
- Nath J, Jambherkar K, Rao C, Armitano E. Radiological and pathological changes in hemiballism-hemichorea with striatal hyperintensity. J Magn Reson Imaging. 2006;23(4):564–68. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources