

Phase II Trial of Erlotinib during and after Radiotherapy in Children with Newly Diagnosed High-Grade Gliomas
- PMID: 24744992
- PMCID: PMC3978340
- DOI: 10.3389/fonc.2014.00067
Phase II Trial of Erlotinib during and after Radiotherapy in Children with Newly Diagnosed High-Grade Gliomas
Abstract
Background: Epidermal growth factor receptor is overexpressed in most pediatric high-grade gliomas (HGG). Since erlotinib had shown activity in adults with HGG, we conducted a phase II trial of erlotinib and local radiotherapy (RT) in children with newly diagnosed HGG.
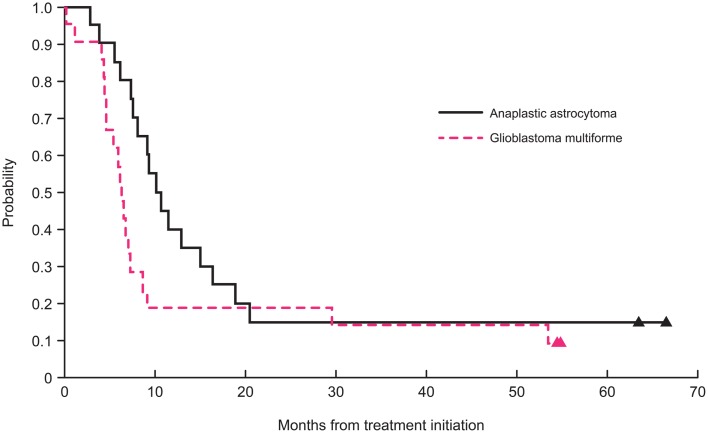
Methods: Following maximum surgical resection, patients between 3 and 21 years with non-metastatic HGG received local RT at 59.4 Gy (54 Gy for spinal tumors and those with ≥70% brain involvement). Erlotinib started on day 1 of RT (120 mg/m(2) per day) and continued for 2 years unless there was tumor progression or intolerable toxicities. The 2-year progression-free survival (PFS) was estimated for patients with intracranial anaplastic astrocytoma (AA) and glioblastoma (GBM).
Results: Median age at diagnosis for 41 patients with intracranial tumors (21 with GBM and 20 with AA) was 10.9 years (range, 3.3-19 years). The 2-year PFS for patients with AA and GBM was 15 ± 7 and 19 ± 8%, respectively. Only five patients remained alive without tumor progression. Twenty-six patients had at least one grade 3 or 4 toxicity irrespective of association with erlotinib; only four required dose modifications. The main toxicities were gastrointestinal (n = 11), dermatologic (n = 5), and metabolic (n = 4). One patient with gliomatosis cerebri who required prolonged corticosteroids died of septic shock associated with pancreatitis.
Conclusion: Although therapy with erlotinib was mostly well-tolerated, it did not change the poor outcome of our patients. Our results showed that erlotinib is not a promising medication in the treatment of children with intracranial AA and GBM.
Keywords: epidermal growth factor receptor; erlotinib; high-grade glioma; pediatric; phase II; radiotherapy.
Figures
References
-
- Finlay JL, Boyett JM, Yates AJ, Wisoff JH, Milstein JM, Geyer JR, et al. Randomized phase III trial in childhood high-grade astrocytoma comparing vincristine, lomustine, and prednisone with the eight-drugs-in-1-day regimen. Children’s Cancer Group. J Clin Oncol (1995) 13:112–23 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials