

Safety and tolerability of inhaled loxapine in subjects with asthma and chronic obstructive pulmonary disease--two randomized controlled trials
- PMID: 24745666
- PMCID: PMC4273199
- DOI: 10.1089/jamp.2013.1114
Safety and tolerability of inhaled loxapine in subjects with asthma and chronic obstructive pulmonary disease--two randomized controlled trials
Abstract
Background: Loxapine, a first-generation antipsychotic, delivered with a novel inhalation delivery device developed for the acute treatment of agitation in patients with schizophrenia or bipolar disorder was evaluated in subjects with asthma or chronic obstructive pulmonary disease (COPD).
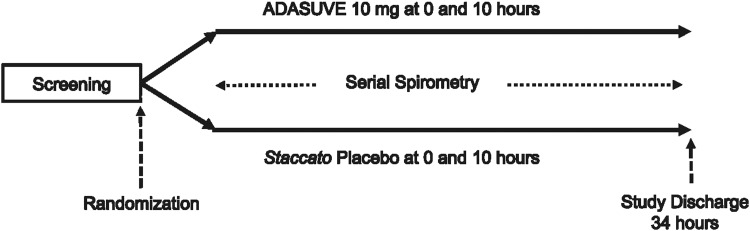
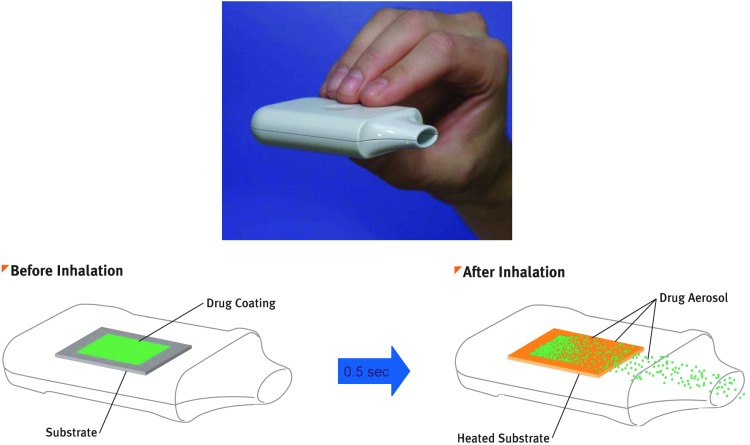
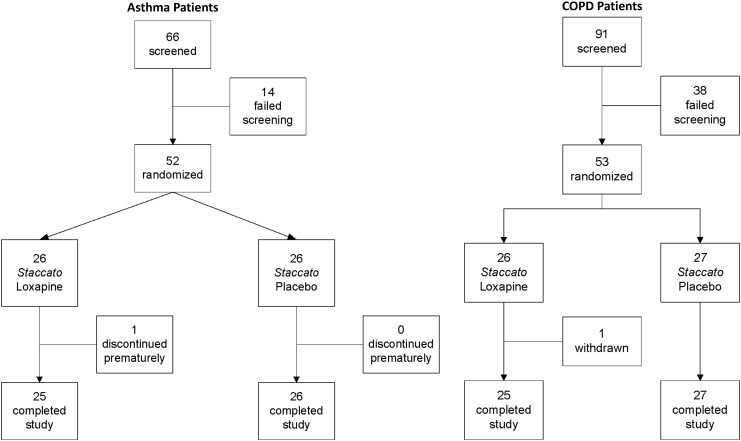
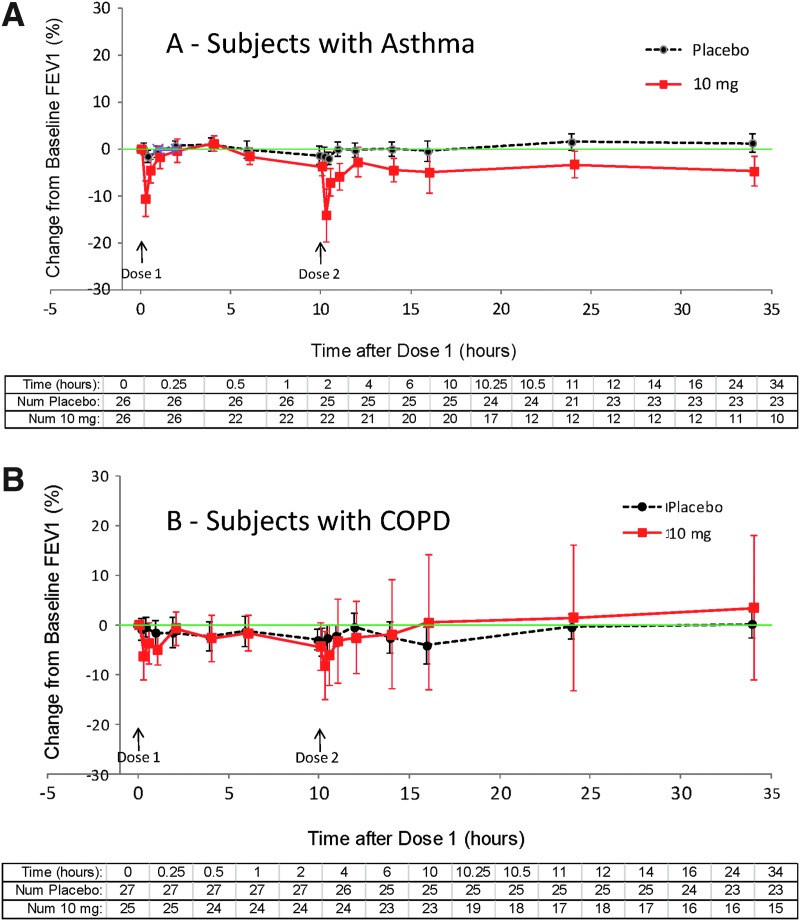
Methods: Separate randomized, double-blind, parallel-arm, placebo-controlled trials compared two administrations of inhaled loxapine (10 mg) 10 hr apart with placebo in 52 subjects with asthma and in 53 subjects with COPD. A thermally-generated drug aerosol of loxapine was delivered to the deep lung for rapid systemic absorption. Controller medications were continued throughout the study, but quick-relief bronchodilators were withheld from 6-8 hr before through 34 hr after dose 1, unless indicated as rescue.
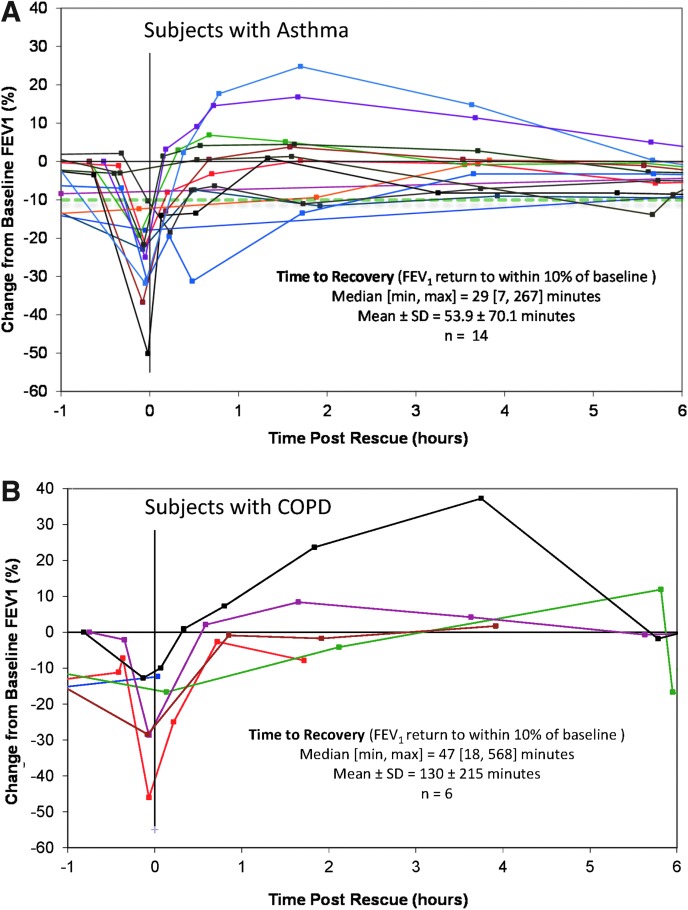
Results: All airway adverse events (AEs) were of mild or moderate severity. Symptomatic bronchospasm occurred in 53.8% of subjects with asthma after inhaled loxapine and 11.5% after placebo; and in 19.2% of COPD subjects after inhaled loxapine and 11.1% after placebo. Subjects required inhaled albuterol as follows: asthma: 53.8% after inhaled loxapine and 11.5% after placebo; and COPD: 23.1% after inhaled loxapine and 14.8% after placebo. Respiratory signs/symptoms requiring treatment responded to rescue bronchodilator [forced expiratory volume in 1 sec (FEV(1)) return to within 10% of baseline] within 1 hr in 11 of 15 events in asthma subjects and four of seven events in COPD subjects, the remainder by the last spirometry.
Conclusions: In subjects with either asthma or COPD, FEV(1) decline and bronchospasm can occur following inhaled loxapine, but more frequently in asthmatic subjects. Most subjects with bronchospasm responded to rescue bronchodilator within 1 hr. No treatment-related serious AE occurred. Although inhaled loxapine is contraindicated in patients with active airways disease per the current approved US labeling, these studies demonstrated that rescue bronchodilator mitigated the symptomatic bronchospasms that may occur in case of inadvertent use.
Trial registration: ClinicalTrials.gov NCT00889837 NCT00890175.
Keywords: ADASUVE; COPD; aerosol; agitation; asthma; inhaled loxapine; randomized; safety.
Figures
References
-
- Heel RC, Brogden RN, Speight TM, and Avery GS: Loxapine: a review of its pharmacological properties and therapeutic efficacy as an antipsychotic agent. Drugs. 1978;15:198–217 - PubMed
-
- Paprocki J, and Versiani M: A double-blind comparison between loxapine and haloperidol by parenteral route in acute schizophrenia. Curr Ther Res Clin Exp. 1977;21:80–100 - PubMed
-
- Fruensgaard K, Korsgaard S, Jorgensen H, and Jensen K: Loxapine versus haloperidol parenterally in acute psychosis with agitation. A double-blind study. Acta Psychiatr Scand. 1977;56:256–264 - PubMed
-
- Dubin WR, and Weiss KJ: Rapid tranquilization: a comparison of thiothixene with loxapine. J Clin Psychiatry. 1986;47:294–297 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
