

Evolution of the hip fracture population: time to consider the future? A retrospective observational analysis
- PMID: 24747789
- PMCID: PMC3996816
- DOI: 10.1136/bmjopen-2013-004405
Evolution of the hip fracture population: time to consider the future? A retrospective observational analysis
Abstract
Objective: To examine how the population with fractured neck of femur has changed over the last decade and determine whether they have evolved to become a more physically and socially dependent cohort.
Design: Retrospective cohort study of prospectively collected Standardised Audit of Hip Fractures of Europe data entered on to an institutional hip fracture registry.
Participants: 10 044 consecutive hip fracture admissions (2000-2012).
Setting: A major trauma centre in the UK.
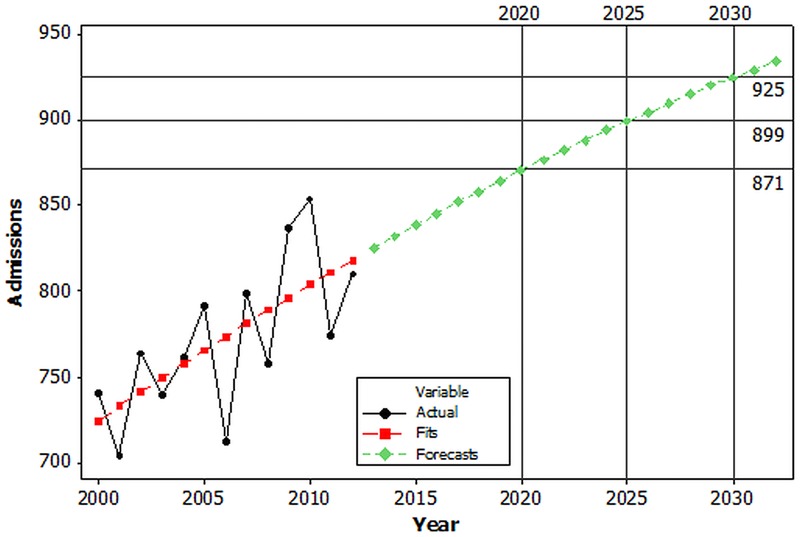
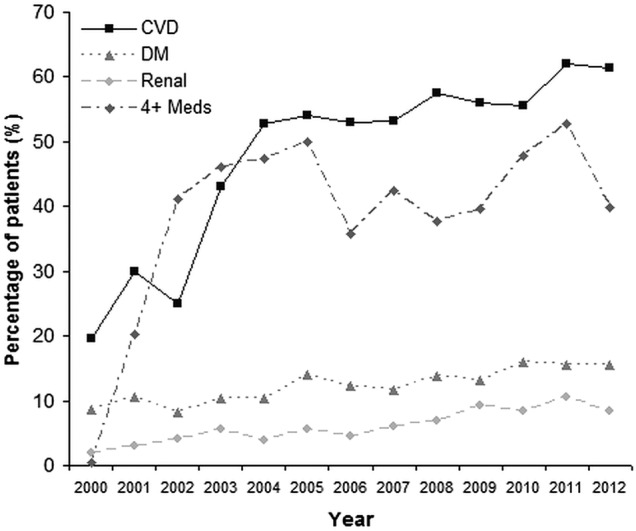
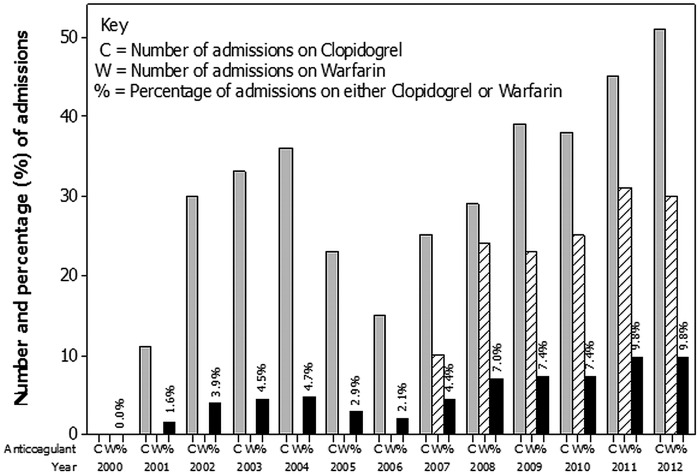
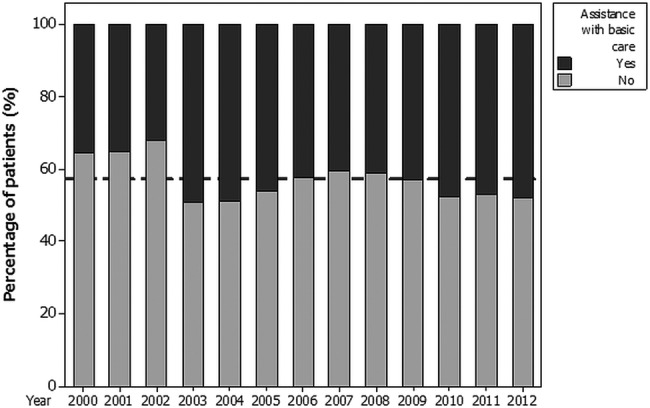
Results: There was a generalised increase in the number of admissions between 2000 (n=740) and 2012 (n=810). This increase was non-linear and best described by a quadratic curve. Assuming no change in the prevalence of hip fracture over the next 20 years, our hospital is projected to treat 871 cases in 2020 and 925 in 2030. This represents an approximate year-on-year increase of just over 1%. There was an increase in the proportion of male admissions over the study period (2000: 174 of 740 admissions (23.5%); 2012: 249 of 810 admissions (30.7%)). This mirrored national census changes within the geographical area during the same period. During the study period there were significant increases in the numbers of patients admitted from their own home, the proportion of patients requiring assistance to mobilise, and the proportion of patients requiring help with basic activities of daily living (all p<0.001). There was also a twofold to fourfold increase in the proportion of patients admitted with a diagnosis of cardiovascular disease, renal disease, diabetes and polypharmacy (use of >4 prescribed medications; all p<0.001).
Conclusions: The expanding hip fracture population has increasingly complex medical, social and rehabilitation care needs. This needs to be recognised so that appropriate healthcare strategies and service planning can be implemented. This epidemiological analysis allows projections of future service need in terms of patient numbers and dependency.
Figures
References
-
- 2011. Hip Fracture. Costing report. Implementing NICE guidance. National Institute for Health and Care Excellence clinical guideline 124.
-
- 2006. Osteoporosis Facts and Figures v1.1 The National Osteoporosis Society publication.
-
- Johansen A, Wakeman R, Boulton C, et al. National report 2013. Clinical Effectiveness and Evaluation Unit, Royal College of Physicians. National Hip Fracture Database.
-
- Quah C, Boulton C, Moran C. The influence of socioeconomic status on the incidence, outcome and mortality of fractures of the hip. J Bone Joint Surg (Br) 2011;93-B:801–5 - PubMed
-
- White SM, Griffiths R. Projected incidence of proximal femoral fractures in England: a report from the NHS Hip Fracture Anaesthesia Network (HIPFAN). Injury 2011;42:1230–3 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases