

Induction of A. fumigatus-specific CD4-positive T cells in patients recovering from invasive aspergillosis
- PMID: 24747947
- PMCID: PMC4077089
- DOI: 10.3324/haematol.2013.098830
Induction of A. fumigatus-specific CD4-positive T cells in patients recovering from invasive aspergillosis
Abstract
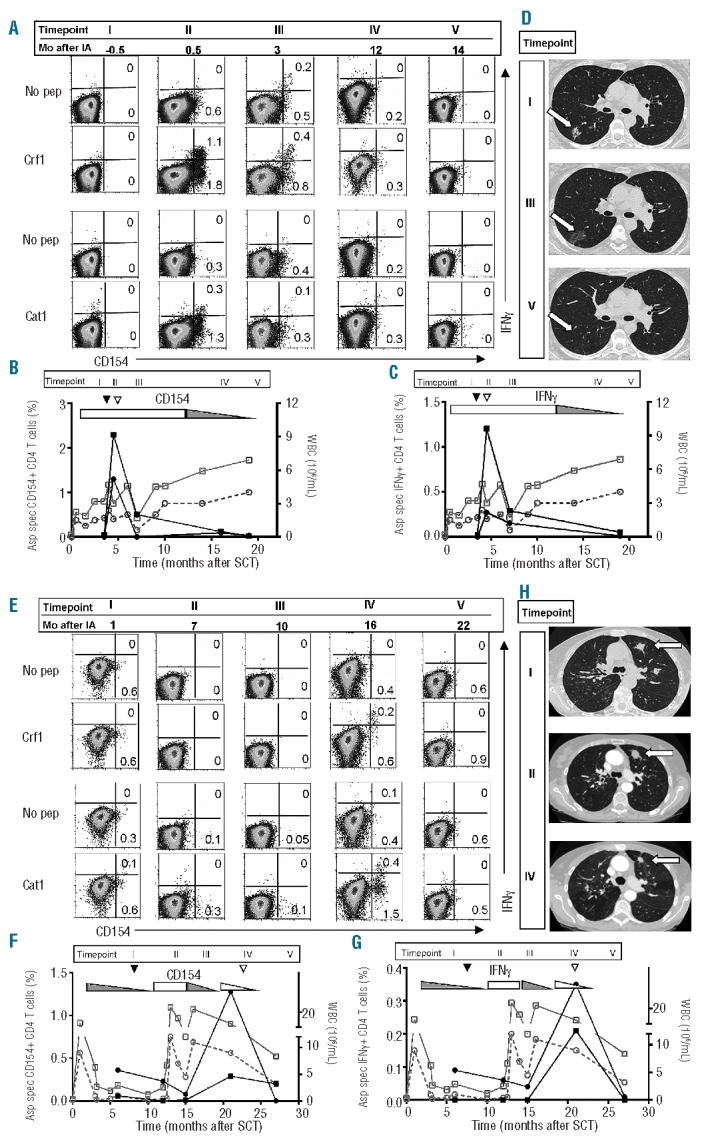
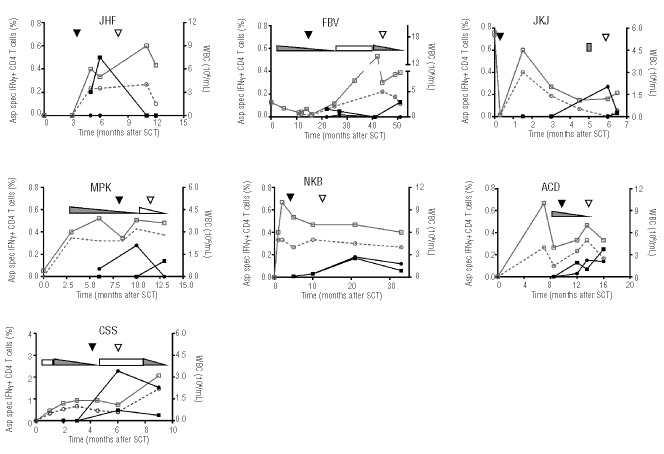
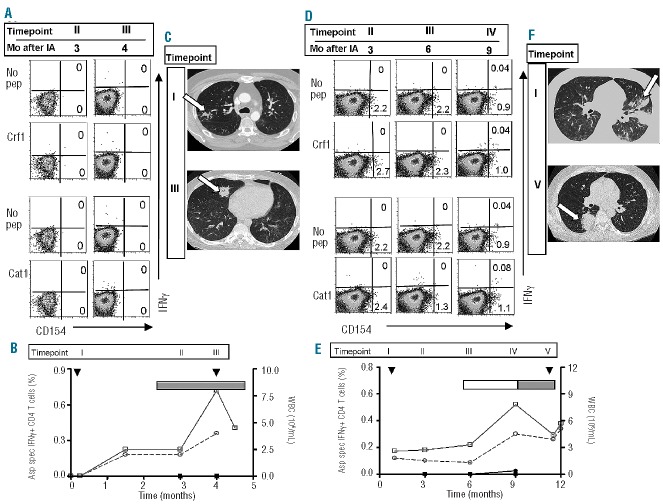
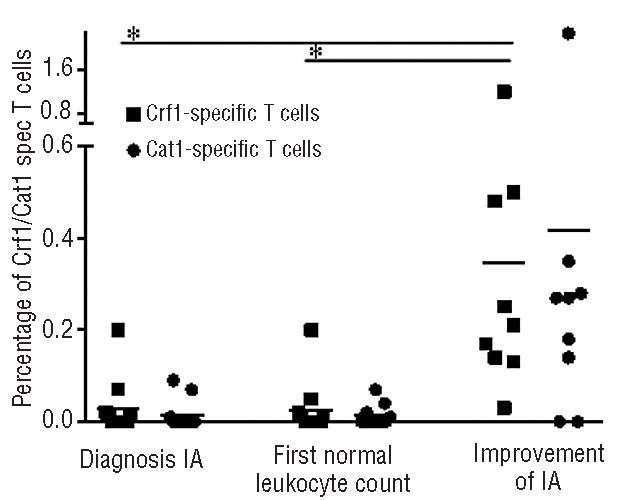
After allogeneic stem cell transplantation patients are at risk of invasive aspergillosis, especially during the period of neutropenia. Recent data suggest that impaired T-cell immune reconstitution after transplantation plays an important role in this increased risk. In this study we investigated whether Aspergillus-specific T cells are involved in the recovery from invasive aspergillosis by analyzing the Aspergillus-specific T-cell response in patients with invasive aspergillosis. In nine patients whose Aspergillus infection improved, we identified Crf1- or Catalase1-specific T cells on the basis of CD154 expression and interferon-γ production following stimulation with overlapping peptides of the A. fumigatus proteins Crf1 and Catalase1. These Aspergillus-specific T cells were induced at the moment of regression of the aspergillus lesions. Crf1- and Catalase1-specific T cells, sorted on the basis of CD154 expression at the peak of the immune response, had a T helper-1 phenotype and recognized a variety of T-cell epitopes. In contrast, in two patients with progressive invasive aspergillosis, no Crf1- or Catalase1-specific T cells were identified. These data indicate that the presence of Aspergillus-specific T cells with a T helper-1 phenotype correlates with the clearance of aspergillus infection.
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Pagano L, Caira M, Nosari A, Van Lint MT, Candoni A, Offidani M, et al. Fungal infections in recipients of hematopoietic stem cell transplants: results of the SEIFEM B-2004 study – Sorveglianza epidemiologica infezioni fungine nelle emopatie maligne. Clin Inf Dis. 2007;45(9):1161–70 - PubMed
-
- Bozza S, Gaziano R, Lipford GB, Montagnoli C, Bacci A, di Francesco P, et al. Vaccination of mice against invasive aspergillosis with recombinant Aspergillus proteins and CpG oligodeoxynucleotides as adjuvants. Microbes Infect. 2002;4(13):1281–90 - PubMed
-
- Bozza S, Perruccio K, Montagnoli C, Gaziano R, Bellocchio S, Burchielli E, et al. A dendritic cell vaccine against invasive aspergillosis in allogeneic hematopoietic transplantation. Blood. 2003;102(10):3807–14 - PubMed
-
- Cenci E, Mencacci A, Bacci A, Bistoni F, Kurup VP, Romani L. T cell vaccination in mice with invasive pulmonary aspergillosis. J Immunol. 2000;165(1):381–8 - PubMed
-
- Hebart H, Bollinger C, Fisch P, Sarfati J, Meisner C, Baur M, et al. Analysis of T-cell responses to Aspergillus fumigatus antigens in healthy individuals and patients with hematologic malignancies. Blood. 2002;100(13):4521–8 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
