

Clinical efficacy and safety of nerve-sparing radical hysterectomy for cervical cancer: a systematic review and meta-analysis
- PMID: 24748015
- PMCID: PMC3991621
- DOI: 10.1371/journal.pone.0094116
Clinical efficacy and safety of nerve-sparing radical hysterectomy for cervical cancer: a systematic review and meta-analysis
Erratum in
- PLoS One. 2014;9(6):e101068
Abstract
Backgroud and objective: Nerve-sparing radical hysterectomy (NSRH) may be associated with lower postoperative morbidity than radical hysterectomy (RH). We aimed to compare the clinical efficacy and safety of abdominal or laparoscopic NSRH and RH for treating cervical cancer through systematic review and meta-analysis.
Methods: PubMed, EMBASE, The Cochrane Library and the Chinese National Knowledge Infrastructure databases were systematically searched for all relevant studies. Data were abstracted independently by two reviewers. A meta-analysis was performed to compare intra- and postoperative outcomes for the two techniques.
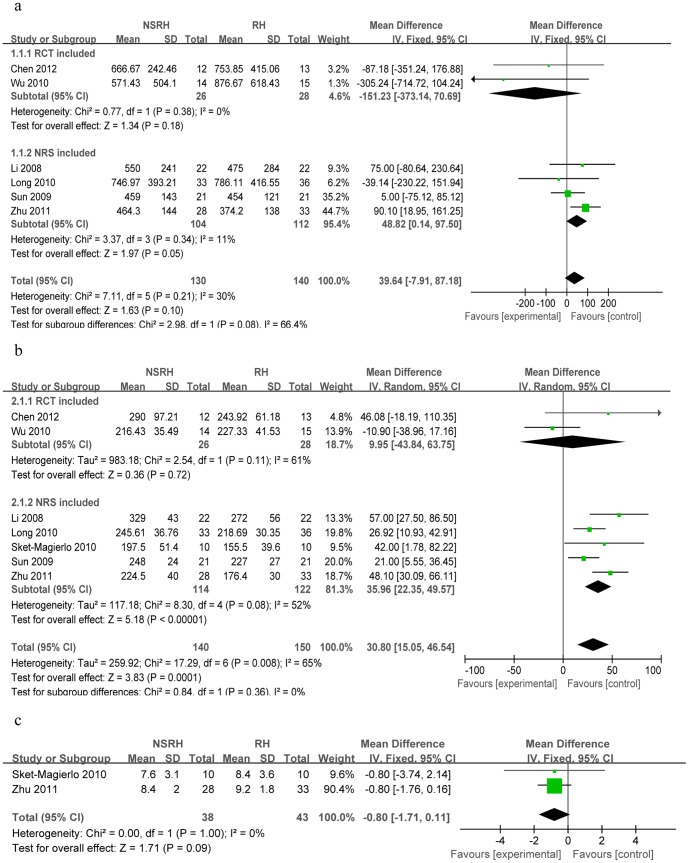
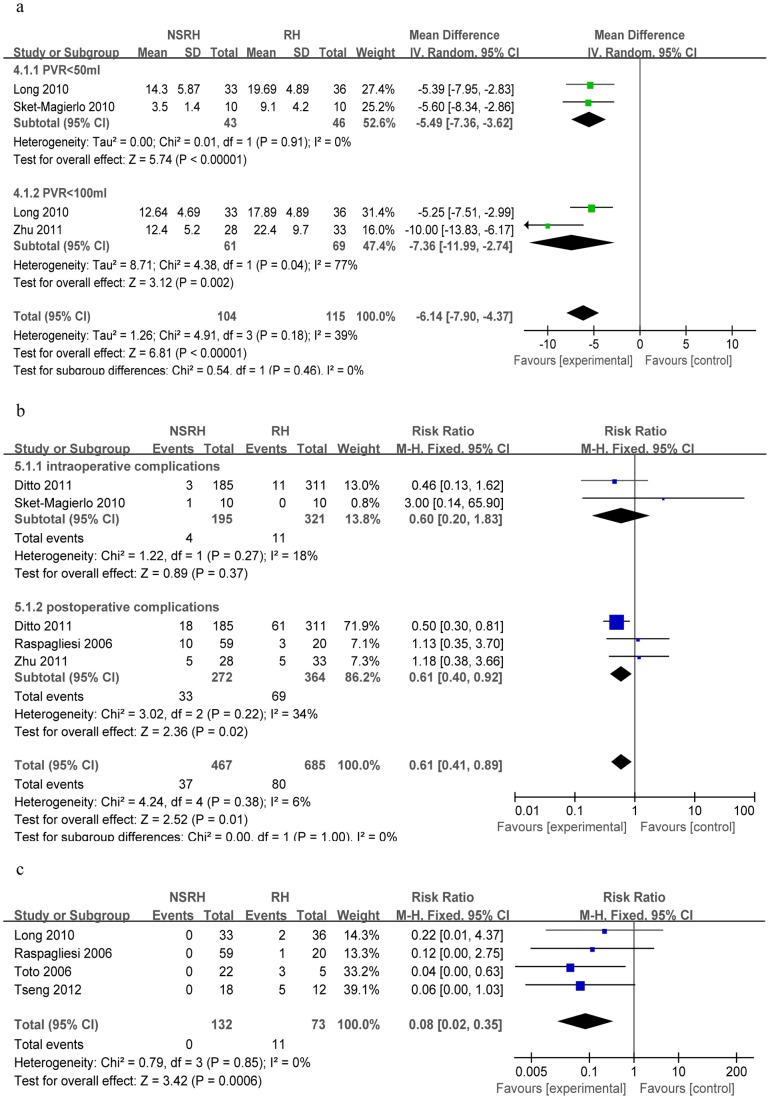
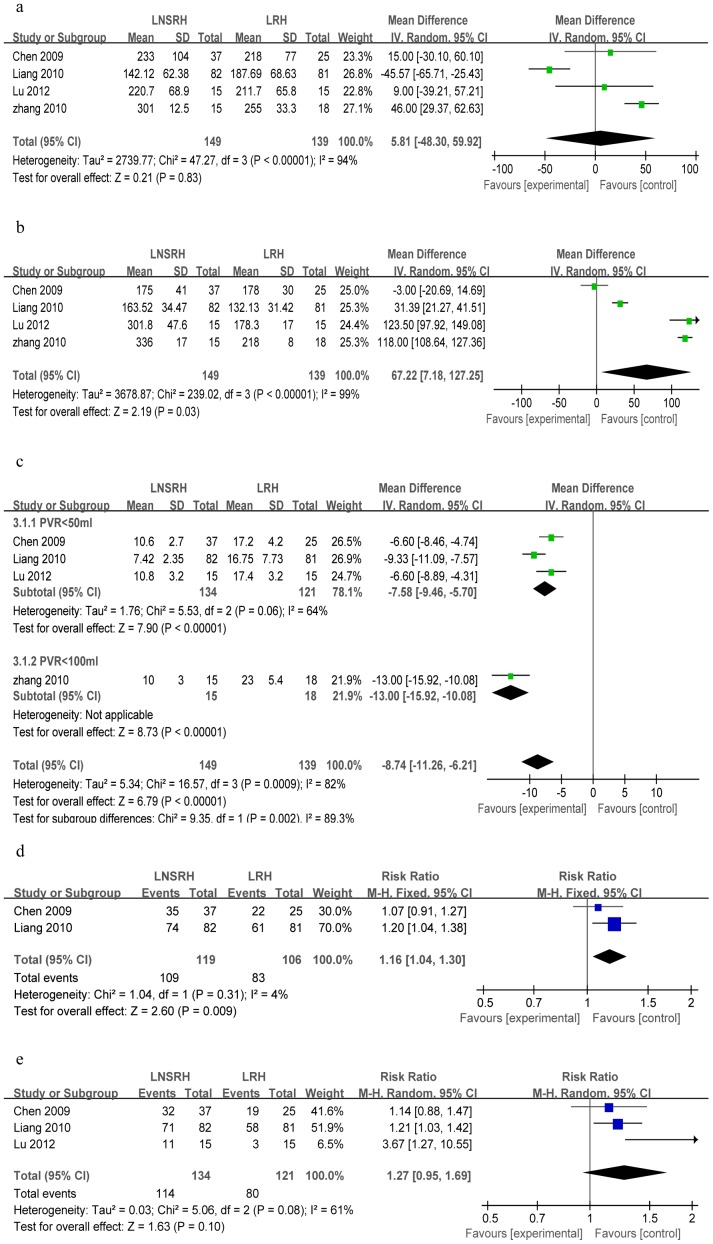
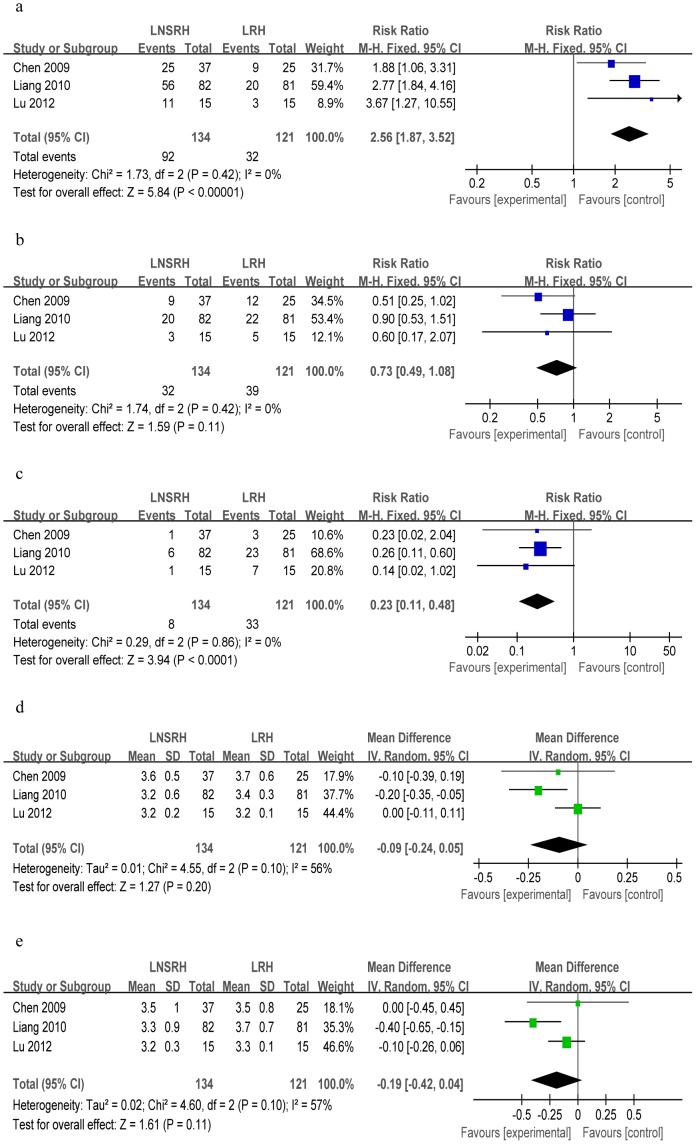
Results: A total of 17 clinical trials were identified. Meta-analysis showed that although operating time was significantly longer for abdominal or laparoscopic NSRH than for RH, NSRH based on laparotomy or laparoscopy proved more effective for postoperative recovery of bladder function. NSRH was also associated with lower bladder dysfunction morbidity and fewer postoperative complications. Two abdominal trials and one laparoscopic study further suggested that NSRH was associated with shorter time to recovery of anal/rectal function. In contrast, RH and NSRH based on laparotomy or laparoscopy were similar in terms of extent of resection, recurrence rate, survival rate, blood loss and frequency of intraoperative complications. The meta-analysis showed that abdominal NSRH was not significantly different from RH in length of hospital stay, while one trial suggested that length of hospital stay was shorter after laparoscopic NSRH than after the corresponding RH.
Conclusion: NSRH may be a reliable technique for treating early cervical cancer. Available evidence suggests that it is better than RH for postoperative recovery of pelvic organ function and postoperative morbidity, while the two techniques involve similar clinical safety and extent of resection. These results should be considered preliminary since they are based on a relatively small number of controlled trials, most of which were non-randomized. The findings should be verified in larger, well-designed studies.
Conflict of interest statement
Figures

References
-
- Bergmark K, Avall-Lundqvist E, Dickman PW, Henningsohn L, Steineck G (1999) Vaginal changes and sexuality in women with a history of cervical cancer. N Engl J Med Overseas Ed 340: 1383–1389. - PubMed
-
- Zullo MA, Manci N, Angioli R, Muzii L, Panici PB (2003) Vesical dysfunctions after radical hysterectomy for cervical cancer: a critical review. Crit Rev Oncol Hematol 48: 287–293. - PubMed
-
- Maas CP, Trimbos JB, DeRuiter MC, van de Velde CJ, Kenter GG (2003) Nerve sparing radical hysterectomy: latest developments and historical perspective. Crit Rev Oncol Hematol 48: 271–279. - PubMed
-
- Watson M, Saraiya M, Benard V, Coughlin SS, Flowers L, et al. (2008) Burden of cervical cancer in the United States, 1998–2003. Cancer 113: 2855–2864. - PubMed
-
- Puntambekar SP, Palep RJ, Puntambekar SS, Wagh GN, Patil AM, et al. (2007) Laparoscopic total radical hysterectomy by the Pune technique: our experience of 248 cases. J Minim Invasive Gynecol 14: 682–689. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
