

The cost-effectiveness of wound-edge protection devices compared to standard care in reducing surgical site infection after laparotomy: an economic evaluation alongside the ROSSINI trial
- PMID: 24748154
- PMCID: PMC3991705
- DOI: 10.1371/journal.pone.0095595
The cost-effectiveness of wound-edge protection devices compared to standard care in reducing surgical site infection after laparotomy: an economic evaluation alongside the ROSSINI trial
Abstract
Background: Wound-edge protection devices (WEPDs) have been used in surgery for more than 40 years to reduce surgical site infection (SSI). No economic evaluation of WEPDs against any comparator has ever been conducted. The aim of the paper was to assess whether WEPDs are cost-effective in reducing SSI compared to standard care alone in the United Kingdom.
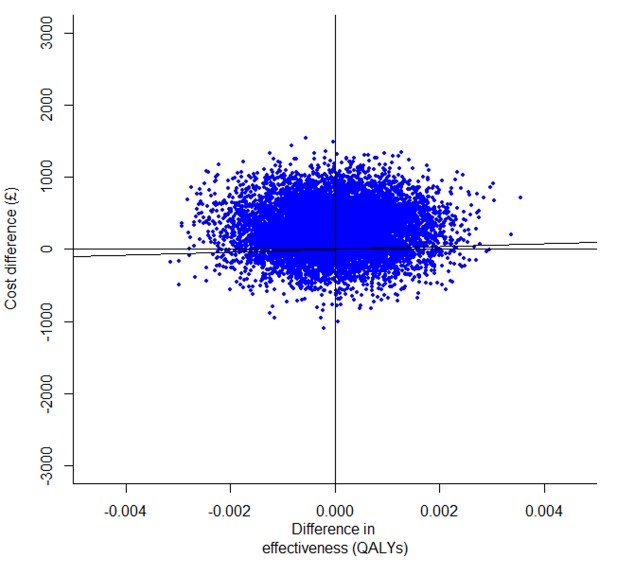
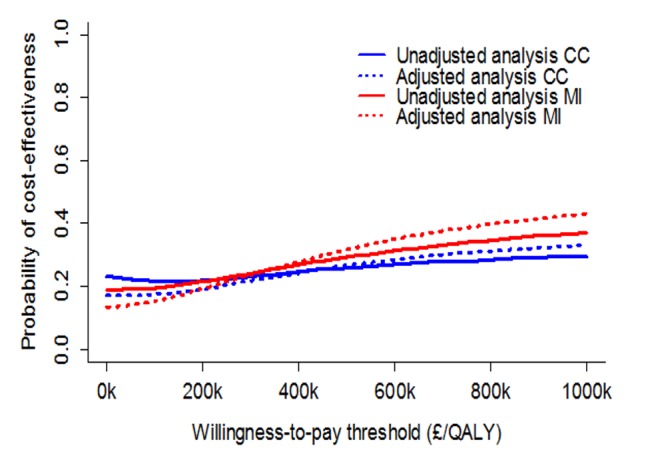
Methods and findings: An economic evaluation was conducted alongside the ROSSINI trial. The study perspective was that of the UK National Health Service and the time horizon was 30 days post-operatively. The study was conducted in 21 UK hospitals. 760 patients undergoing laparotomy were randomised to either WEPD or standard care and 735 were included in the primary analysis. The main economic outcome was cost-effectiveness based on incremental cost (£) per quality adjusted life year (QALY) gained. Patients in the WEPD arm accessed health care worth £5,420 on average and gained 0.02131 QALYs, compared to £5,130 and 0.02133 QALYs gained in the standard care arm. The WEPD strategy was more costly and equally effective compared to standard care, but there was significant uncertainty around incremental costs and QALYs. The findings were robust to a range of sensitivity analyses.
Conclusions: There is no evidence to suggest that WEPDs can be considered a cost effective device to reduce SSI. Their continued use is a waste of limited health care resources.
Conflict of interest statement
Figures
References
-
- Smyth ETM, McIlvenny G, Enstone JE, Emmerson AM, Humphreys H, et al. (2008) Four country healthcare associated infection prevalence survey 2006: overview of the results. J Hosp Infect 69: 230–248. - PubMed
-
- Bruce J, Russell EM, Mollison J, Krukowski ZH (2001) The measurement and monitoring of surgical adverse events. Health Technology Assessment 5: 1–194. - PubMed
-
- Mangram AJ, Horan TC, Pearson ML (1999) Silver LC, Jarvis WR. Guideline for prevention of surgical site infection. American Journal of Infection Control 27: 97–132. - PubMed
-
- Coello R, Charlett A, Wilson J, Ward V, Pearson A, et al. (2005) Adverse impact of surgical site infections in English hospitals. J Hosp Infect 60: 93–103. - PubMed
-
- Tanner J, Khan D, Aplin C, Ball J, Thomas M, et al. (2009) Post-discharge surveillance to identify colorectal surgical site infection rates and related costs. J Hosp Infect 72: 243–250. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
