

Hospital and geographic variability in two colorectal cancer surgery outcomes: complications and mortality after complications
- PMID: 24748161
- PMCID: PMC4090776
- DOI: 10.1245/s10434-013-3472-x
Hospital and geographic variability in two colorectal cancer surgery outcomes: complications and mortality after complications
Abstract
Background: The purpose of this study was to describe hospital and geographic variation in 30-day risk of surgical complications and death among colorectal cancer (CRC) patients and the extent to which patient-, hospital-, and census-tract-level characteristics increased risk of these outcomes.
Methods: We included patients at least 66 years old with first primary stage I-III CRC from the 2000-2005 National Cancer Institute's Surveillance, Epidemiology, and End Results data linked with 1999-2005 Medicare claims. A multilevel, cross-classified logistic model was used to account for nesting of patients within hospitals and within residential census tracts. Outcomes were risk of complications and death after a complication within 30 days of surgery.
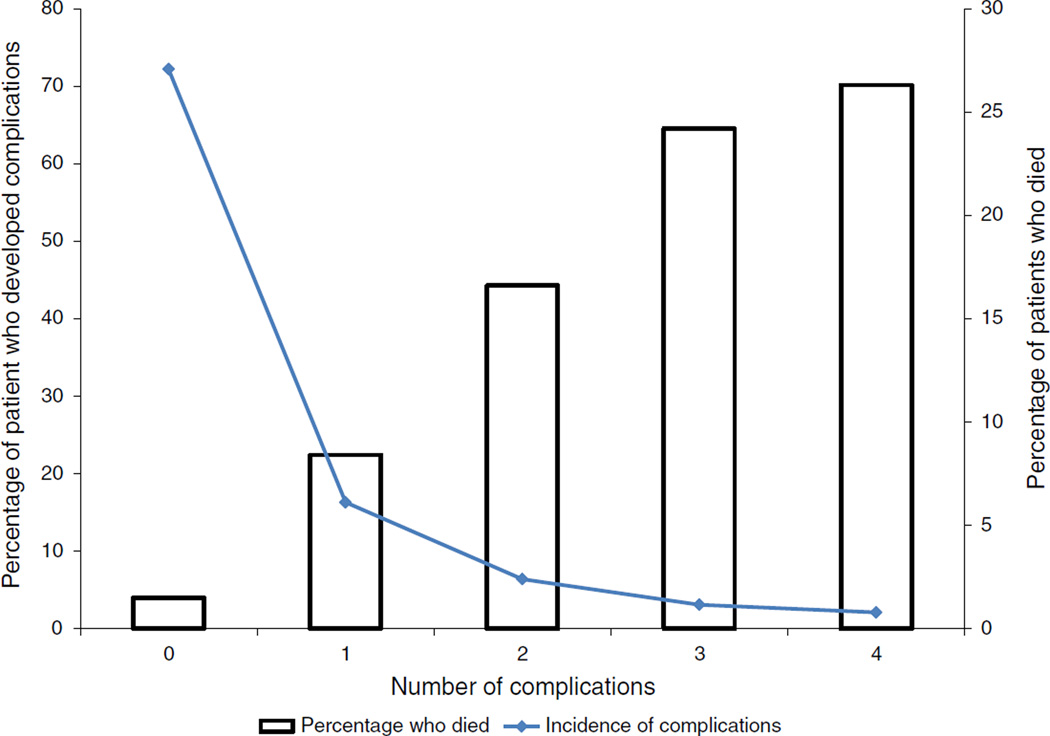
Results: Data were analyzed for 35,946 patients undergoing surgery at 1,222 hospitals and residing in 12,187 census tracts; 27.2 % of patients developed complications, and of these 13.4 % died. Risk-adjusted variability in complications across hospitals and census tracts was similar. Variability in mortality was larger than variability in complications, across hospitals and across census tracts. Specific characteristics increased risk of complications (e.g., census-tract-poverty rate, emergency surgery, and being African-American). No hospital characteristics increased complication risk. Specific characteristics increased risk of death (e.g. census-tract-poverty rate, being diagnosed with colon (versus rectal) cancer, and emergency surgery), while hospitals with at least 500 beds showed reduced death risk.
Conclusions: Large, unexplained variations exist in mortality after surgical complications in CRC across hospitals and geographic areas. The potential exists for quality improvement efforts targeted at the hospital and/or census-tract levels to prevent complications and augment hospitals' ability to reduce mortality risk.
Figures
References
-
- Cancer facts and figures. Atlanta: American Cancer Society; 2012. American Cancer Society. 2012.
-
- Panis Y, Maggiori L, Caranhac G, Bretagnol F, Vicaut E. Mortality after colorectal cancer surgery: a French survey of more than 84,000 patients. Ann Surg. 2011;254:738–743. (discussion 43-4) - PubMed
-
- Fazio VW, Tekkis PP, Remzi F, Lavery IC. Assessment of operative risk in colorectal cancer surgery: the Cleveland Clinic Foundation colorectal cancer model. Dis Colon Rectum. 2004;47:2015–2024. - PubMed
-
- Morris EJ, Taylor EF, Thomas JD, Quirke P, Finan PJ, Coleman MP, et al. Thirty-day postoperative mortality after colorectal cancer surgery in England. Gut. 2011;60:806–813. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
