

Four types of barriers to adherence of antiretroviral therapy are associated with decreased adherence over time
- PMID: 24748240
- PMCID: PMC4203705
- DOI: 10.1007/s10461-014-0775-2
Four types of barriers to adherence of antiretroviral therapy are associated with decreased adherence over time
Abstract
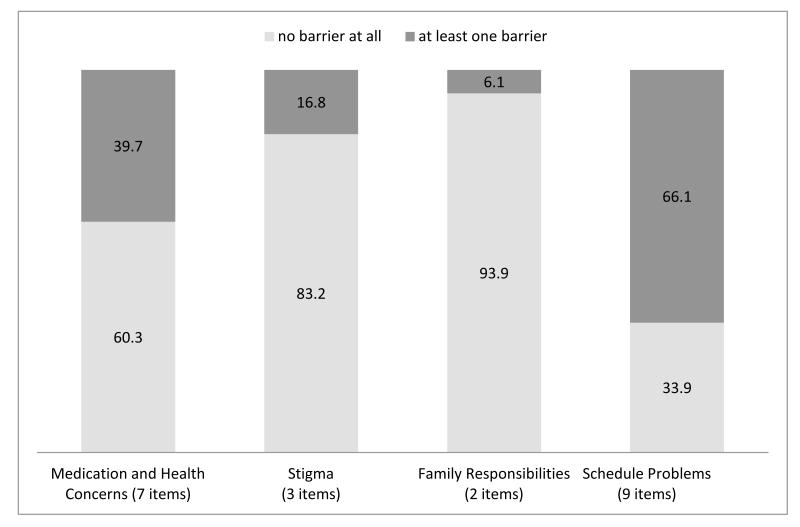
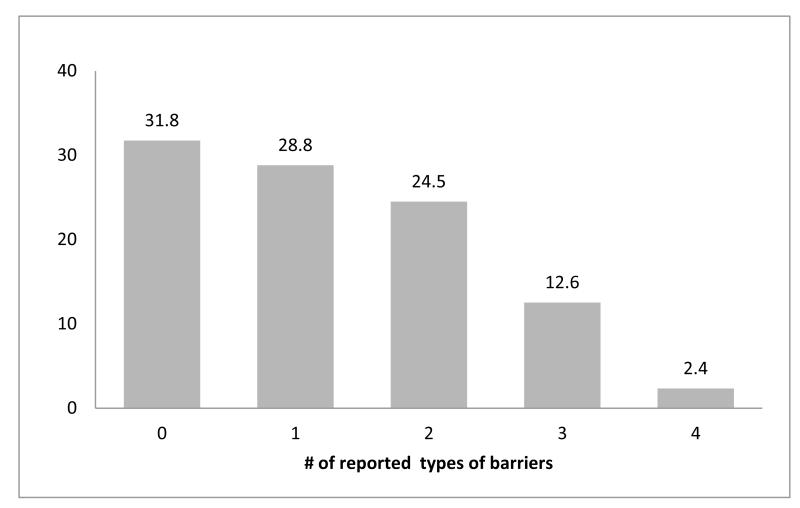
The objectives of this study were to understand how different types of barriers to adherence to antiretroviral therapy (ART) were related and their differential impact on objectively measured adherence over time. Data from 151 patients taking ART were used to describe four sub-types of self-reported adherence barriers: medication and health concerns (MHC), stigma (S), family responsibilities (FR), and problems with schedule and routine (PSR). Generalized linear models with generalized estimating equations (GEE) were used to examine the impact of barriers on adherence over time. The sample was 23 % female, mean age 42 years, with 26 % African-American and 20 % Hispanic. The overall average adherence was 73 %. Patients reported at least one PSR barrier in 66 % of study visits, MHC in 40 %, S in 17 %, and FR in 6 %. In 40 % of visits, patients reported two or more barrier sub-types. There were statistically significant (p ≤ 0.05) decreases of 3.9, 2.5, and 2.4 in percent adherence, for MHC, PSR, and S, respectively, per unit increase in barrier score. Interventions to address different types of patient-identified barriers to ART adherence using targeted approaches are needed.
Figures
References
-
- Bangsberg DR, Perry S, Charlebois ED, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. AIDS. 2001;15(9):1181–1183. - PubMed
-
- Ammassari A, Trotta MP, Murri R, et al. Correlates and predictors of adherence to highly active antiretroviral therapy: overview of published literature. J Acquir Immune Defic Syndr. 2002;31(Suppl 3):S123–7. - PubMed
-
- Chesney M. Adherence to HAART regimens. AIDS Patient Care STDS. 2003;17(4):169–177. - PubMed
-
- Fogarty L, Roter D, Larson S, Burke J, Gillespie J, Levy R. Patient adherence to HIV medication regimens: a review of published and abstract reports. Patient Educ Couns. 2002;46(2):93–108. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
