

Dihydroartemisinin-piperaquine vs. artemether-lumefantrine for first-line treatment of uncomplicated malaria in African children: a cost-effectiveness analysis
- PMID: 24748395
- PMCID: PMC3991722
- DOI: 10.1371/journal.pone.0095681
Dihydroartemisinin-piperaquine vs. artemether-lumefantrine for first-line treatment of uncomplicated malaria in African children: a cost-effectiveness analysis
Abstract
Background: Recent multi-centre trials showed that dihydroartemisinin-piperaquine (DP) was as efficacious and safe as artemether-lumefantrine (AL) for treatment of young children with uncomplicated P. falciparum malaria across diverse transmission settings in Africa. Longitudinal follow-up of patients in these trials supported previous findings that DP had a longer post-treatment prophylactic effect than AL, reducing the risk of reinfection and conferring additional health benefits to patients, particularly in areas with moderate to high malaria transmission.
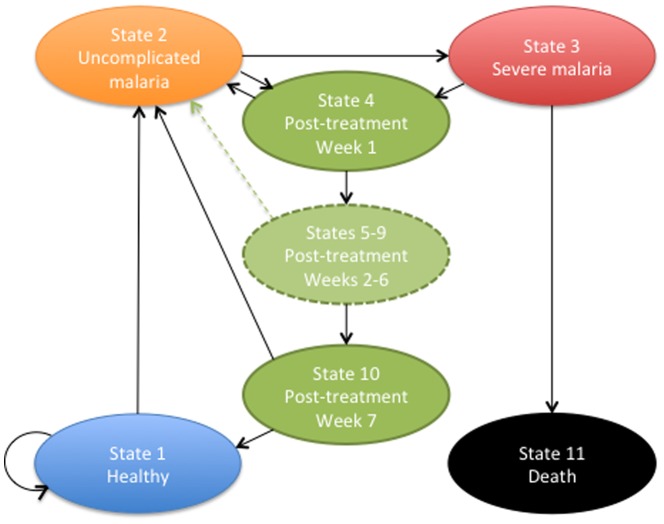
Methods: We developed a Markov model to assess the cost-effectiveness of DP versus AL for first-line treatment of uncomplicated malaria in young children from the provider perspective, taking into consideration the post-treatment prophylactic effects of the drugs as reported by a recent multi-centre trial in Africa and using the maximum manufacturer drug prices for artemisinin-based combination therapies set by the Global Fund in 2013. We estimated the price per course of treatment threshold above which DP would cease to be a cost-saving alternative to AL as a first-line antimalarial drug.
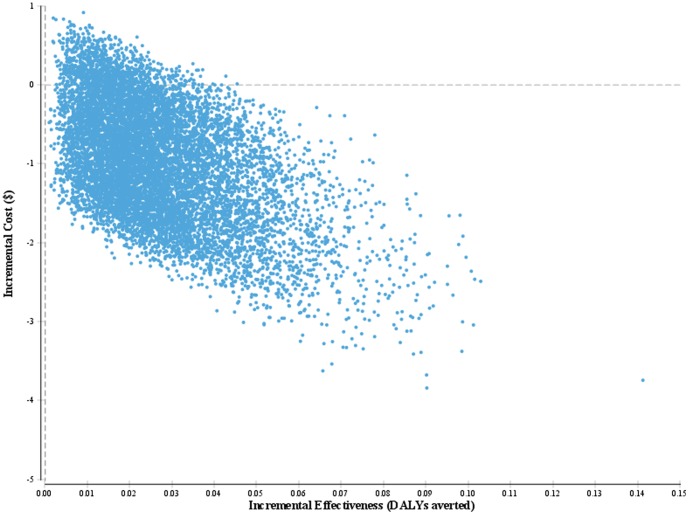
Results: First-line treatment with DP compared to AL averted 0.03 DALYs (95% CI: 0.006-0.07) and 0.001 deaths (95% CI: 0.00-0.002) and saved $0.96 (95% CI: 0.33-2.46) per child over one year. The results of the threshold analysis showed that DP remained cost-saving over AL for any DP cost below $1.23 per course of treatment.
Conclusions: DP is superior to AL from both the clinical and economic perspectives for treatment of uncomplicated P. falciparum malaria in young children. A paediatric dispersible formulation of DP is under development and should facilitate a targeted deployment of this antimalarial drug. The use of DP as first-line antimalarial drug in paediatric malaria patients in moderate to high transmission areas of Africa merits serious consideration by health policymakers.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
