

Outcomes of an innovative model of acute delirium care: the Geriatric Monitoring Unit (GMU)
- PMID: 24748778
- PMCID: PMC3986297
- DOI: 10.2147/CIA.S60259
Outcomes of an innovative model of acute delirium care: the Geriatric Monitoring Unit (GMU)
Abstract
Objective: Delirium is associated with poor outcomes following acute hospitalization. The Geriatric Monitoring Unit (GMU) is a specialized five-bedded unit for acute delirium care. It is modeled after the Delirium Room program, with adoption of core interventions from the Hospital Elder Life Program and use of evening light therapy to consolidate circadian rhythms and improve sleep in older inpatients. This study examined whether the GMU program improved outcomes in delirious patients.
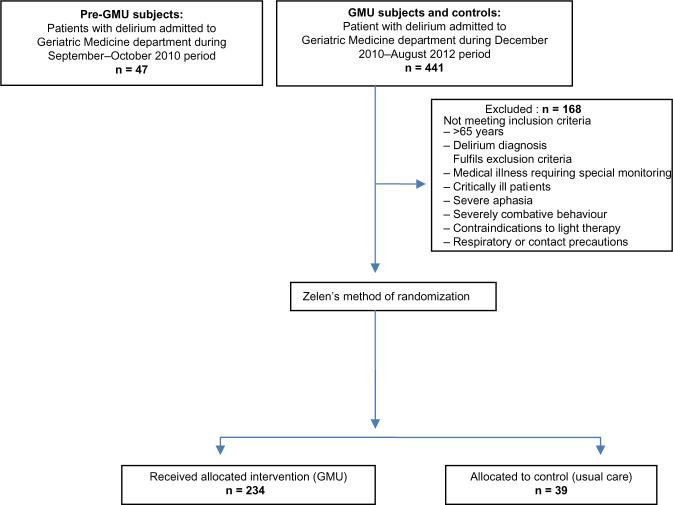
Method: A total of 320 patients, including 47 pre-GMU, 234 GMU, and 39 concurrent control subjects, were studied. Clinical characteristics, cognitive status, functional status (Modified Barthel Index [MBI]), and chemical restraint-use data were obtained. We also looked at in-hospital complications of falls, pressure ulcers, nosocomial infection rate, and discharge destination. Secondary outcomes of family satisfaction (for the GMU subjects) were collected.
Results: There were no significant demographic differences between the three groups. Pre-GMU subjects had longer duration of delirium and length of stay. MBI improvement was most evident in the GMU compared with pre-GMU and control subjects (19.2±18.3, 7.5±11.2, 15.1±18.0, respectively) (P<0.05). The GMU subjects had a zero restraint rate, and pre-GMU subjects had higher antipsychotic dosages. This translated to lower pressure ulcer and nosocomial infection rate in the GMU (4.1% and 10.7%, respectively) and control (1.3% and 7.7%, respectively) subjects compared with the pre-GMU (9.1% and 23.4%, respectively) subjects (P<0.05). No differences were observed in mortality or discharge destination among the three groups. Caregivers of GMU subjects felt the multicomponent intervention to be useful, with scheduled activities voted the most beneficial in patient's recovery from the delirium episode.
Conclusion: This study shows the benefits of a specialized delirium management unit for older persons. The GMU model is thus a relevant system of care for rapidly "graying" nations with high rates of frail elderly hospital admissions, which can be easily transposed across acute care settings.
Keywords: delirium; elderly; function.
Figures
Similar articles
-
A new model of delirium care in the acute geriatric setting: geriatric monitoring unit.BMC Geriatr. 2011 Aug 13;11:41. doi: 10.1186/1471-2318-11-41. BMC Geriatr. 2011. PMID: 21838912 Free PMC article. Clinical Trial.
-
Bright light therapy as part of a multicomponent management program improves sleep and functional outcomes in delirious older hospitalized adults.Clin Interv Aging. 2013;8:565-72. doi: 10.2147/CIA.S44926. Epub 2013 May 22. Clin Interv Aging. 2013. PMID: 23723696 Free PMC article.
-
Functional improvement in hospitalized older adults is independent of dementia diagnosis: experience of a specialized delirium management unit.J Hosp Med. 2013 Jun;8(6):321-7. doi: 10.1002/jhm.2035. Epub 2013 Mar 29. J Hosp Med. 2013. PMID: 23553979
-
Non-Pharmacological Interventions to Prevent or Treat Delirium in Older Patients: Clinical Practice Recommendations The SENATOR-ONTOP Series.J Nutr Health Aging. 2016;20(9):927-936. doi: 10.1007/s12603-016-0719-9. J Nutr Health Aging. 2016. PMID: 27791223 Review.
-
A review of recent clinical trials and guidelines on the prevention and management of delirium in hospitalized older patients.Hosp Pract (1995). 2011 Oct;39(4):96-106. doi: 10.3810/hp.2011.10.928. Hosp Pract (1995). 2011. PMID: 22056829 Review.
Cited by
-
Comprehensive geriatric assessment in the emergency department.Clin Interv Aging. 2014 Nov 24;9:2033-43. doi: 10.2147/CIA.S29662. eCollection 2014. Clin Interv Aging. 2014. PMID: 25473275 Free PMC article. Review.
-
Agitation and Dementia: Prevention and Treatment Strategies in Acute and Chronic Conditions.Front Neurol. 2021 Apr 16;12:644317. doi: 10.3389/fneur.2021.644317. eCollection 2021. Front Neurol. 2021. PMID: 33935943 Free PMC article. Review.
-
Changing Hospital Care For Older Adults: The Case for Geriatric Hospitals in the United States.Gerontol Geriatr Med. 2022 Jul 4;8:23337214221109005. doi: 10.1177/23337214221109005. eCollection 2022 Jan-Dec. Gerontol Geriatr Med. 2022. PMID: 35813982 Free PMC article.
-
Impact of a dementia-friendly program on detection and management of patients with cognitive impairment and delirium in acute-care hospital units: a controlled clinical trial design.BMC Geriatr. 2022 Mar 31;22(1):266. doi: 10.1186/s12877-022-02949-0. BMC Geriatr. 2022. PMID: 35361136 Free PMC article. Clinical Trial.
-
Postoperative delirium: identifying the patient at risk and altering the course: A narrative review.Eur J Anaesthesiol Intensive Care. 2023 Apr 26;2(3):e0022. doi: 10.1097/EA9.0000000000000022. eCollection 2023 Jun. Eur J Anaesthesiol Intensive Care. 2023. PMID: 39917289 Free PMC article. Review.
References
-
- Agnostini JV, Inouye Sk. Delirium. In: Hazzard WR, Blass JP, Halter JB, Ouslander JG, Tinetti ME, editors. Principles in Geriatric Medicine and Gerontology. 5th ed. New York, NY: McGraw-Hill; 2003. pp. 1503–1515.
-
- Inouye SK. Delirium in hospitalized older patients. Clin Geriatr Med. 1998;14(4):745–764. - PubMed
-
- Moran JA, Dorevitch MI. Delirium in the hospitalized elderly. Australian Journal of Hospital Pharmacy. 2001;31:35–40.
-
- Murray AM, Levkoff SE, Wetle TT, et al. Acute delirium and functional decline in the hospitalized elderly patient. J Gerontol. 1993;48(5):M181–M186. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
