

No evidence of real progress in treatment of acute pain, 1993-2012: scientometric analysis
- PMID: 24748816
- PMCID: PMC3990387
- DOI: 10.2147/JPR.S60842
No evidence of real progress in treatment of acute pain, 1993-2012: scientometric analysis
Abstract
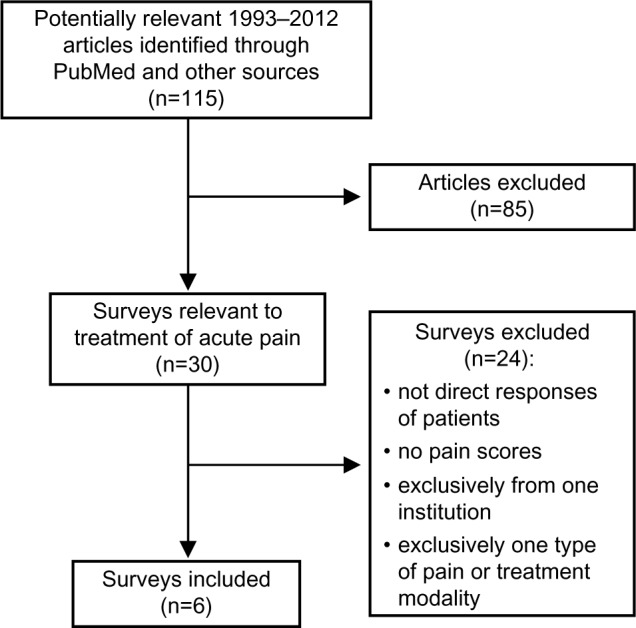
Over the past 2 decades, many new techniques and drugs for the treatment of acute pain have achieved widespread use. The main aim of this study was to assess the progress in their implementation using scientometric analysis. The following scientometric indices were used: 1) popularity index, representing the share of articles on a specific technique (or a drug) relative to all articles in the field of acute pain; 2) index of change, representing the degree of growth in publications on a topic compared to the previous period; and 3) index of expectations, representing the ratio of the number of articles on a topic in the top 20 journals relative to the number of articles in all (>5,000) biomedical journals covered by PubMed. Publications on specific topics (ten techniques and 21 drugs) were assessed during four time periods (1993-1997, 1998-2002, 2003-2007, and 2008-2012). In addition, to determine whether the status of routine acute pain management has improved over the past 20 years, we analyzed surveys designed to be representative of the national population that reflected direct responses of patients reporting pain scores. By the 2008-2012 period, popularity index had reached a substantial level (≥5%) only with techniques or drugs that were introduced 30-50 years ago or more (epidural analgesia, patient-controlled analgesia, nerve blocks, epidural analgesia for labor or delivery, bupivacaine, and acetaminophen). In 2008-2012, promising (although modest) changes of index of change and index of expectations were found only with dexamethasone. Six national surveys conducted for the past 20 years demonstrated an unacceptably high percentage of patients experiencing moderate or severe pain with not even a trend toward outcome improvement. Thus, techniques or drugs that were introduced and achieved widespread use for acute pain management within the past 20 years have produced no changes in scientometric indices that would indicate real progress and have failed to improve national outcomes for relief of acute pain. Two possible reasons for this are discussed: 1) the difference between the effectiveness of old and new techniques is not clinically meaningful; and 2) resources necessary for appropriate use of new techniques in routine pain management are not adequate.
Keywords: continuous nerve block; epidural analgesia; multimodal analgesia; nerve block; pain management; patient-controlled epidural analgesia; patient-controlled intravenous analgesia; postoperative pain.
Figures
References
Supplementary material
List of articles on the treatment of acute pain, 1993–2012
-
- Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97:534–540. - PubMed
-
- Bamigboye AA, Hofmeyr GJ. Local anaesthetic wound infiltration and abdominal nerves block during caesarean section for postoperative pain relief. Cochrane Database Syst Rev. 2009;(3):CD006954. - PubMed
-
- Barletta JF. Clinical and economic burden of opioid use for postsurgical pain: focus on ventilatory impairment and ileus. Pharmacotherapy. 2012;32(Suppl 9):12S–18S. - PubMed
-
- Benhamou D, Berti M, Brodner G, et al. Postoperative Analgesic THerapy Observational Survey (PATHOS); a practice pattern study in 7 central/southern European countries. Pain. 2008;136:134–141. - PubMed
-
- Block BM, Liu SS, Rowlingson AJ, Cowan AR, Cowan JA, Jr, Wu CL. Efficacy of postoperative epidural analgesia: a meta-analysis. JAMA. 2003;290:2455–2463. - PubMed
References
-
- Acute pain management: operative or medical procedures and trauma, Part 1. Agency for Health Care Policy and Research. Clin Pharm. 1992;11:309–331. [No authors listed] - PubMed
-
- Acute pain management: operative or medical procedures and trauma, Part 2. Agency for Health Care Policy and Research. Clin Pharm. 1992;11:391–414. [No authors listed] - PubMed
-
- Warfield CA, Kahn CH. Acute pain management. Programs in US hospitals and experiences and attitudes among US adults. Anesthesiology. 1995;83:1090–1094. - PubMed
-
- Carr DB, Goudas LC. Acute pain. Lancet. 1999;353(9169):2051–2058. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
