

Two Japanese cases of birt-hogg-dubé syndrome with pulmonary cysts, fibrofolliculomas, and renal cell carcinomas
- PMID: 24748863
- PMCID: PMC3985789
- DOI: 10.1159/000358216
Two Japanese cases of birt-hogg-dubé syndrome with pulmonary cysts, fibrofolliculomas, and renal cell carcinomas
Abstract
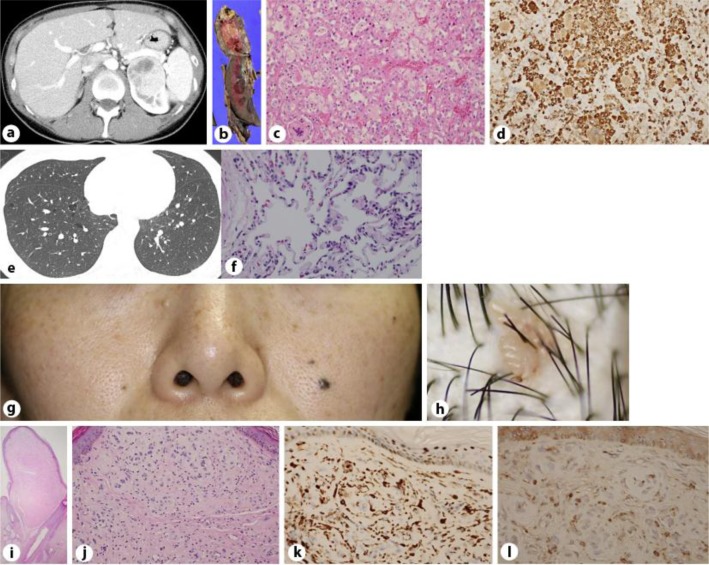
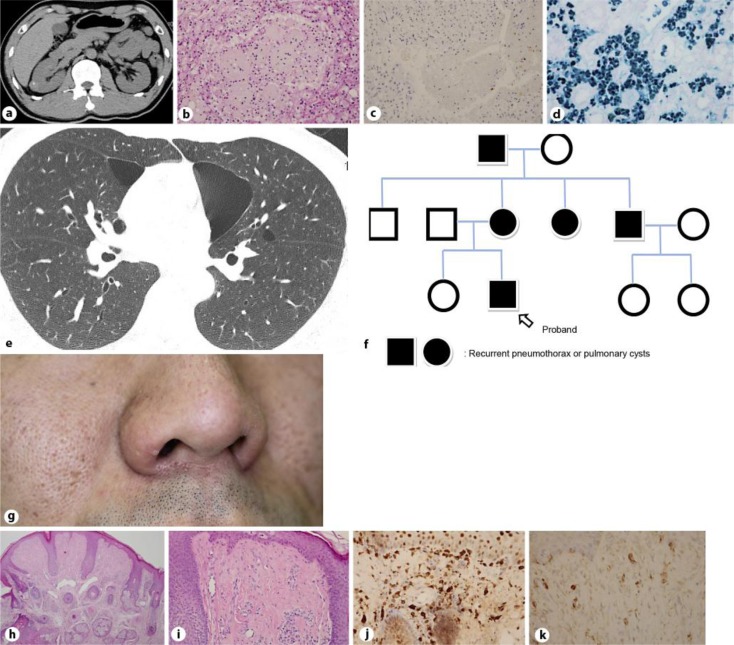
Birt-Hogg-Dubé syndrome (BHD) is a rare autosomal dominant inherited disease caused by a germline mutation in the folliculin gene mapped in the region of chromosome 17p11.2. BHD predisposes the patient to cutaneous fibrofolliculomas (FFs), pulmonary cysts (PCs), and renal cell carcinoma (RC). Here, we present two cases of BHD in Japanese patients. One patient was a 37-year-old female, and the other a 35-year-old male. Each of the patients was affected by all three symptoms of BHD. Both patients had unremarkable FFs, asymptomatic PCs, and asymptomatic RC. The presence of RC was revealed by abdominal ultrasonic examination. We also summarized the data from 62 Asian cases of BHD from the available literature and found that their FFs were unremarkable. In addition, the proportion of BHD patients with FF is smaller for Asian patients than it is for Caucasian patients. We also found that it is rare for BHD patients in Asia to show all three symptoms of BHD. Careful inspection of the skin as well as skin biopsies are important for the early detection of BHD cases in Asia.
Keywords: Birt-Hogg-Dubé syndrome; Fibrofolliculoma; Pulmonary cyst; Renal cell carcinoma.
Figures
References
-
- Menko FH, van Steensel MA, Giraud S, Friis-Hansen L, Richard S, Ungari S, Nordenskjold M, Hansen TV, Solly J, Maher ER, European BHDC Birt-Hogg-Dubé syndrome: diagnosis and management. Lancet Oncol. 2009;10:1199–1206. - PubMed
-
- Kunogi M, Kurihara M, Ikegami TS, Kobayashi T, Shindo N, Kumasaka T, Gunji Y, Kikkawa M, Iwakami S, Hino O, Takahashi K, Seyama K. Clinical and genetic spectrum of Birt-Hogg-Dube syndrome patients in whom pneumothorax and/or multiple lung cysts are the presenting feature. J Med Genet. 2010;47:281–287. - PMC - PubMed
-
- Toro JR, Wei MH, Glenn GM, Weinreich M, Toure O, Vocke C, Turner M, Choyke P, Merino MJ, Pinto PA, Steinberg SM, Schmidt LS, Linehan WM. BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet. 2008;45:321–331. - PMC - PubMed
-
- Pavlovich CP, Grubb RL, 3rd, Hurley K, Glenn GM, Toro J, Schmidt LS, Torres-Cabala C, Merino MJ, Zbar B, Choyke P, Walther MM, Linehan WM. Evaluation and management of renal tumors in the Birt-Hogg-Dubé syndrome. J Urol. 2005;173:1482–1486. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
