

Recent advances in the molecular genetics of type 2 diabetes mellitus
- PMID: 24748926
- PMCID: PMC3990314
- DOI: 10.4239/wjd.v5.i2.128
Recent advances in the molecular genetics of type 2 diabetes mellitus
Abstract
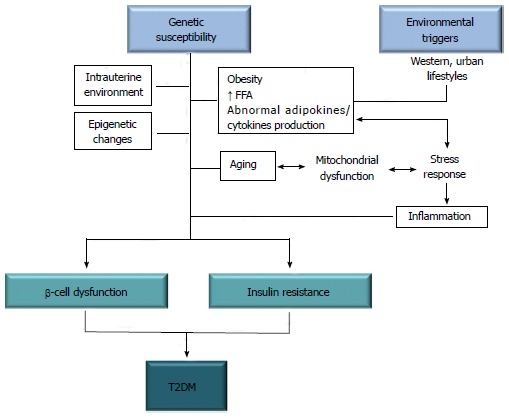
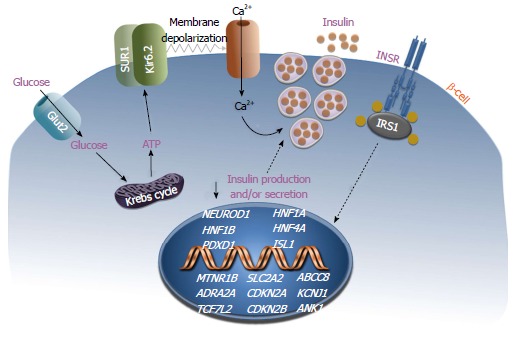
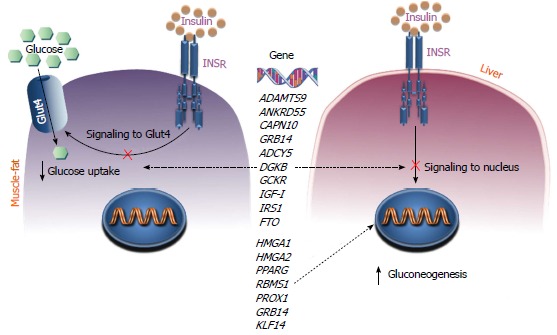
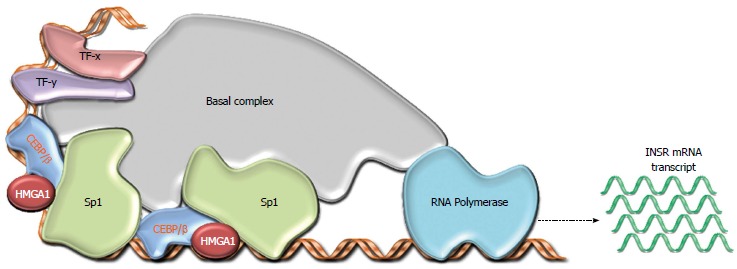
Type 2 diabetes mellitus (T2DM) is a complex disease in which both genetic and environmental factors interact in determining impaired β-cell insulin secretion and peripheral insulin resistance. Insulin resistance in muscle, liver and fat is a prominent feature of most patients with T2DM and obesity, resulting in a reduced response of these tissues to insulin. Considerable evidence has been accumulated to indicate that heredity is a major determinant of insulin resistance and T2DM. It is believed that, among individuals destined to develop T2DM, hyperinsulinemia is the mechanism by which the pancreatic β-cell initially compensates for deteriorating peripheral insulin sensitivity, thus ensuring normal glucose tolerance. Most of these people will develop T2DM when β-cells fail to compensate. Despite the progress achieved in this field in recent years, the genetic causes of insulin resistance and T2DM remain elusive. Candidate gene association, linkage and genome-wide association studies have highlighted the role of genetic factors in the development of T2DM. Using these strategies, a large number of variants have been identified in many of these genes, most of which may influence both hepatic and peripheral insulin resistance, adipogenesis and β-cell mass and function. Recently, a new gene has been identified by our research group, the HMGA1 gene, whose loss of function can greatly raise the risk of developing T2DM in humans and mice. Functional genetic variants of the HMGA1 gene have been associated with insulin resistance syndromes among white Europeans, Chinese individuals and Americans of Hispanic ancestry. These findings may represent new ways to improve or even prevent T2DM.
Keywords: Candidate gene; Genetic variants; Genome-wide association study; High-mobility group A1; Insulin resistant diabetes.
Figures
References
-
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, Lin JK, Farzadfar F, Khang YH, Stevens GA, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet. 2011;378:31–40. doi: 10.1016/S0140-6736(11)60679-X. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
