

Human papillomavirus and cystic node metastasis in oropharyngeal cancer and cancer of unknown primary origin
- PMID: 24752007
- PMCID: PMC3994055
- DOI: 10.1371/journal.pone.0095364
Human papillomavirus and cystic node metastasis in oropharyngeal cancer and cancer of unknown primary origin
Erratum in
- PLoS One. 2014;9(12):e116030
Abstract
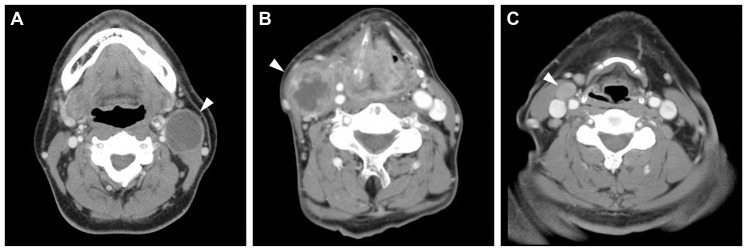
The clinical significance of human papillomavirus (HPV) in neck node metastasis from cancer of unknown primary (CUP) is not well established. We aimed to address the relationship of HPV status between node metastasis and the primary tumor, and also the relevance of HPV status regarding radiographically detected cystic node metastasis in head and neck squamous cell carcinoma (HNSCC) and CUP. HPV DNA was examined in 68 matched pairs of node metastasis and primary tumor, and in node metastasis from 27 CUPs. In surgically treated CUPs, p16 was examined immunohistochemically. When tonsillectomy proved occult tonsillar cancer in CUP, HPV DNA and p16 were also examined in the occult primary. Cystic node metastasis on contrast-enhanced computed tomography scans was correlated with the primary site and HPV status in another series of 255 HNSCCs and CUPs with known HPV status. Node metastasis was HPV-positive in 19/37 (51%) oropharyngeal SCCs (OPSCCs) and 10/27 (37%) CUPs, but not in non-OPSCCs. Fluid was collected from cystic node metastasis using fine needle aspiration in two OPSCCs and one CUP, and all fluid collections were HPV-positive. HPV status, including the presence of HPV DNA, genotype, and physical status, as well as the expression pattern of p16 were consistent between node metastasis and primary or occult primary tumor. Occult tonsillar cancer was found more frequently in p16-positive CUP than in p16-negative CUP (odds ratio (OR), 39.0; 95% confidence interval (CI), 1.4-377.8; P = 0.02). Radiographically, cystic node metastasis was specific to OPSCC and CUP, and was associated with HPV positivity relative to necrotic or solid node metastasis (OR, 6.2; 95% CI, 1.2-45.7; P = 0.03). In conclusion, HPV status remains unchanged after metastasis. The occult primary of HPV-positive CUP is most probably localized in the oropharynx. HPV status determined from fine needle aspirates facilitates the diagnosis of cystic node metastasis.
Conflict of interest statement
Figures

References
-
- Strojan P, Ferlito A, Medina JE, Woolgar JA, Rinaldo A, et al. (2013) Contemporary management of lymph node metastases from an unknown primary to the neck: I. a review of diagnostic approaches. Head Neck 35: 123–132. - PubMed
-
- Cianchetti M, Mancuso AA, Amdur RJ, Werning JW, Kirwan J, et al. (2009) Diagnostic evaluation of squamous cell carcinoma metastatic to cervical lymph nodes from an unknown head and neck primary site. Laryngoscope 119: 2348–2354. - PubMed
-
- Mork J, Lie AK, Glattre E, Jellum E, Koskela P, et al. (2001) Human papillomavirus infection as a risk factor for squamous-cell carcinoma of the head and neck. N Engl J Med 344: 1125–1131. - PubMed
-
- Allen CT, Lewis JS Jr, El-Mofty SK, Haughey BH, Nussenbaum B (2010) Human papillomavirus and oropharynx cancer: biology, detection and clinical implications. Laryngoscope 120: 1756–1772. - PubMed
-
- Begum S, Gillison ML, Ansari-Lari MA, Shah K, Westra WH (2003) Detection of human papillomavirus in cervical lymph nodes: a highly effective strategy for localizing site of tumor origin. Clin Cancer Res 9: 6469–6475. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
