

Meta-analysis of the global gene expression profile of triple-negative breast cancer identifies genes for the prognostication and treatment of aggressive breast cancer
- PMID: 24752235
- PMCID: PMC4007196
- DOI: 10.1038/oncsis.2014.14
Meta-analysis of the global gene expression profile of triple-negative breast cancer identifies genes for the prognostication and treatment of aggressive breast cancer
Erratum in
-
Meta-analysis of the global gene expression profile of triple-negative breast cancer identifies genes for the prognostication and treatment of aggressive breast cancer.Oncogenesis. 2014 Oct 27;3(10):e124. doi: 10.1038/oncsis.2014.41. Oncogenesis. 2014. PMID: 25347059 Free PMC article. No abstract available.
Abstract
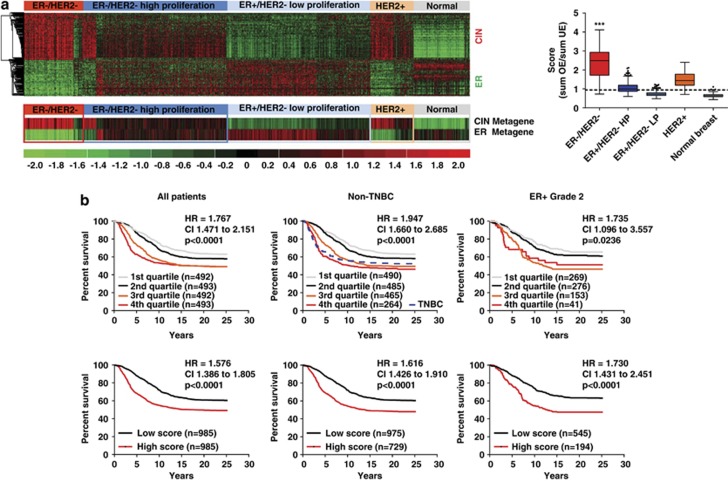
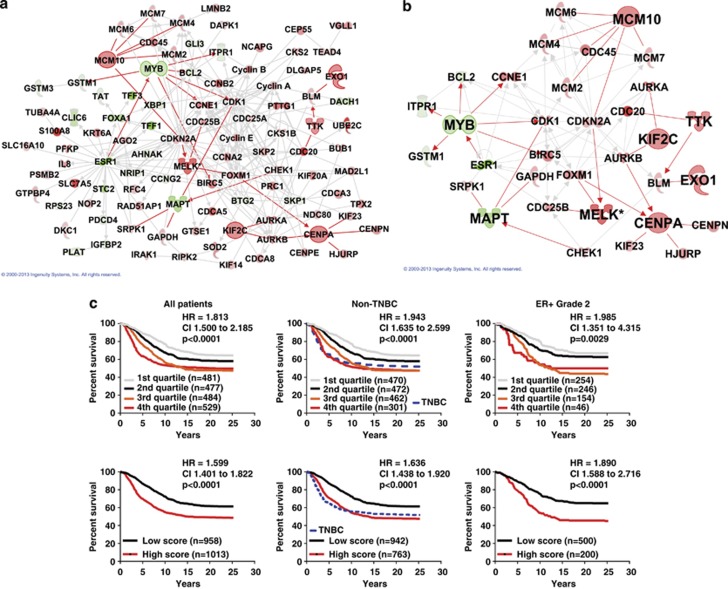
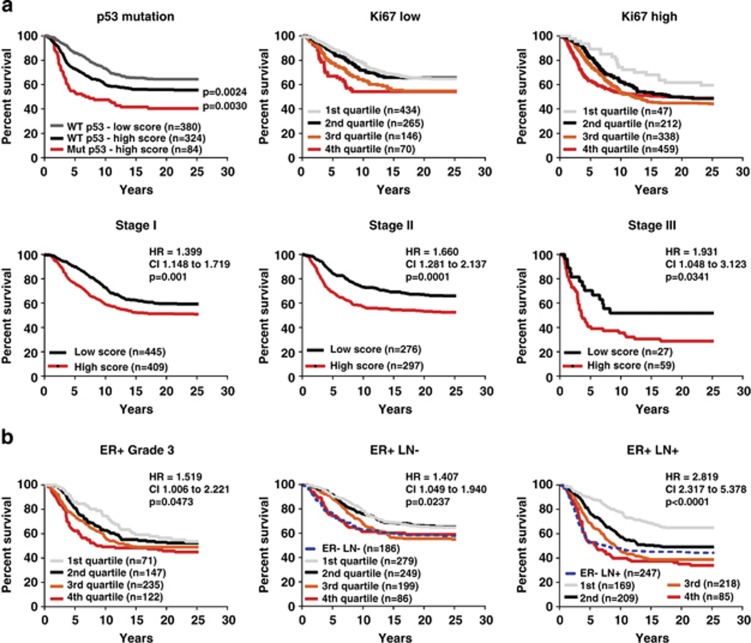
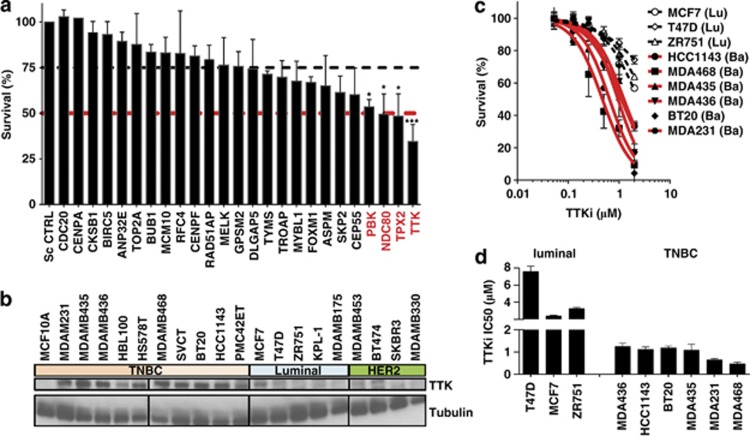
Triple-negative breast cancer (TNBC) is an aggressive breast cancer subtype lacking expression of estrogen and progesterone receptors (ER/PR) and HER2, thus limiting therapy options. We hypothesized that meta-analysis of TNBC gene expression profiles would illuminate mechanisms underlying the aggressive nature of this disease and identify therapeutic targets. Meta-analysis in the Oncomine database identified 206 genes that were recurrently deregulated in TNBC compared with non-TNBC and in tumors that metastasized or led to death within 5 years. This 'aggressiveness gene list' was enriched for two core functions/metagenes: chromosomal instability (CIN) and ER signaling metagenes. We calculated an 'aggressiveness score' as the ratio of the CIN metagene to the ER metagene, which identified aggressive tumors in breast cancer data sets regardless of subtype or other clinico-pathological indicators. A score calculated from six genes from the CIN metagene and two genes from the ER metagene recapitulated the aggressiveness score. By multivariate survival analysis, we show that our aggressiveness scores (from 206 genes or the 8 representative genes) outperformed several published prognostic signatures. Small interfering RNA screen revealed that the CIN metagene holds therapeutic targets against TNBC. Particularly, the inhibition of TTK significantly reduced the survival of TNBC cells and synergized with docetaxel in vitro. Importantly, mitosis-independent expression of TTK protein was associated with aggressive subgroups, poor survival and further stratified outcome within grade 3, lymph node-positive, HER2-positive and TNBC patients. In conclusion, we identified the core components of CIN and ER metagenes that identify aggressive breast tumors and have therapeutic potential in TNBC and aggressive breast tumors. Prognostication from these metagenes at the mRNA level was limited to ER-positive tumors. However, we provide evidence that mitosis-independent expression of TTK protein was prognostic in TNBC and other aggressive breast cancer subgroups, suggesting that protection of CIN/aneuploidy drives aggressiveness and treatment resistance.
Figures



References
-
- Liedtke C, Mazouni C, Hess KR, Andre F, Tordai A, Mejia JA, et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J Clin Oncol. 2008;26:1275–1281. - PubMed
-
- Carey LA, Dees EC, Sawyer L, Gatti L, Moore DT, Collichio F, et al. The triple negative paradox: primary tumor chemosensitivity of breast cancer subtypes. Clin Cancer Res. 2007;13:2329–2334. - PubMed
-
- von Minckwitz G, Untch M, Blohmer JU, Costa SD, Eidtmann H, Fasching PA, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol. 2012;30:1796–1804. - PubMed
-
- Perou CM, Sorlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, et al. Molecular portraits of human breast tumours. Nature. 2000;406:747–752. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
