

Medicare non-payment of hospital-acquired infections: infection rates three years post implementation
- PMID: 24753974
- PMCID: PMC3983733
- DOI: 10.5600/mmrr.003.03.a08
Medicare non-payment of hospital-acquired infections: infection rates three years post implementation
Abstract
Background: Medicare ceased payment for some hospital-acquired infections beginning October 1, 2008, following provisions in the Medicare Modernization Act of 2003 and the Deficit Reduction Act of 2005.
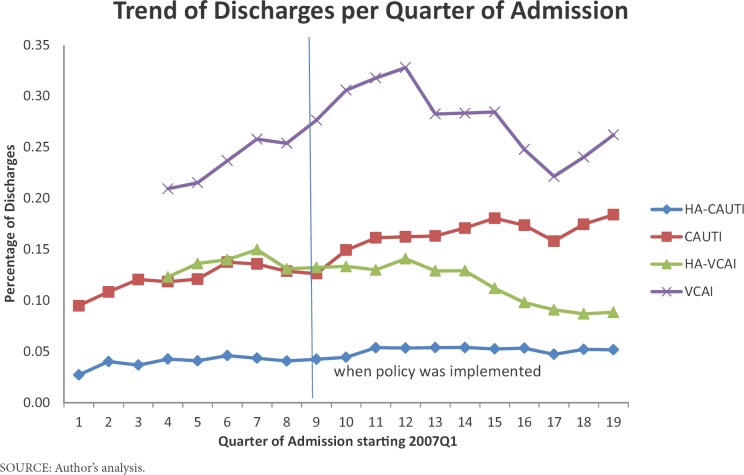
Objective: We examined the association of this policy with declines in rates of vascular catheter-associated infections (VCAI) and catheter-associated urinary tract infection (CAUTI).
Data: Discharge data from the Florida Agency for Healthcare Administration from 2007 to 2011.
Study design: We compared rates of hospital-acquired vascular catheter-associated infections (HA-VCAI) and catheter-associated urinary tract infections (HA-CAUTI) before and after implementation of the new policy (January 2007 to September 2008 vs. October 2008 to September 2011). This pre-post, retrospective, interrupted time series study was further analyzed with a generalized hierarchical logistic regression, by estimating the probability of a patient acquiring these infections in the hospital, post-policy compared to pre-policy.
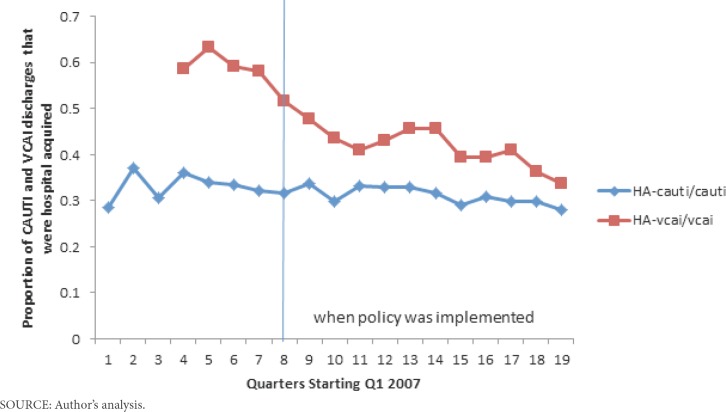
Principal findings: Pre-policy, 0.12% of admitted patients were diagnosed with CAUTI; of these, 32% were HA-CAUTI. Similarly, 0.24% of admissions were diagnosed as VCAI; of these, 60% were HA-VCAI. Post-policy, 0.16% of admissions were CAUTIs; of these, 31% were HA-CAUTI. Similarly, 0.3% of admissions were VCAIs and, of these, 45% were HA-VCAI. There was a statistically significant decrease in HA-VCAIs (OR: 0.571 (p < 0.0001)) post-policy, but the reduction in HA-CAUTI (OR: 0.968 (p < 0.4484)) was not statistically significant.
Conclusions: The results suggest Medicare non payment policy is associated with both a decline in the rate of hospital-acquired VCAI (HA-VCAI) per quarter, and the probability of acquiring HA-VCAI post- policy. The strength of the association could be overestimated, because of concurrent ongoing infection control interventions.
Keywords: Hospital-Acquired Infections; Medicare; Patient Outcomes.
Figures
References
-
- Agency for Health Care Administration. 2010 Retrieved from http://www.floridahealthfinder.gov/Researchers/OrderData/order-data.aspx.
-
- Agency for Healthcare Research and Quality. 2012 Retrieved from http://www.ahrq.gov/news/press/pr2012/pspclabsipr.htm. - PubMed
-
- Apisarnthanarak A, Thongphubeth K, Sirinvaravong S, Kitkangvan D, Yuekyen C, Warachan B, . . .Fraser VJ. The Effectiveness of Multifaceted Hospital Wide Quality Improvement Programs Featuring an Intervention to Remove Unnecessary Urinary Catheters at a Tertiary Care Center in Thailand. Infection Control and Hospital Epidemiology. 2007;28(7):791–798. doi: 10.1086/518453. - DOI - PubMed
-
- Centers for Medicare & Medicaid Services. Eliminating Serious, Preventable, and Costly Medical Errors-Never Events. 2006 Retrieved from http://www.cms.hhs.gov/apps/media/press/release.asp?counter=1863.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical