

Outcomes of out-of-hospital cardiac arrest by public location in the public-access defibrillation era
- PMID: 24755149
- PMCID: PMC4187486
- DOI: 10.1161/JAHA.113.000533
Outcomes of out-of-hospital cardiac arrest by public location in the public-access defibrillation era
Abstract
Background: The strategy to place public-access automated external defibrillators (AEDs) has not yet been established in real settings.
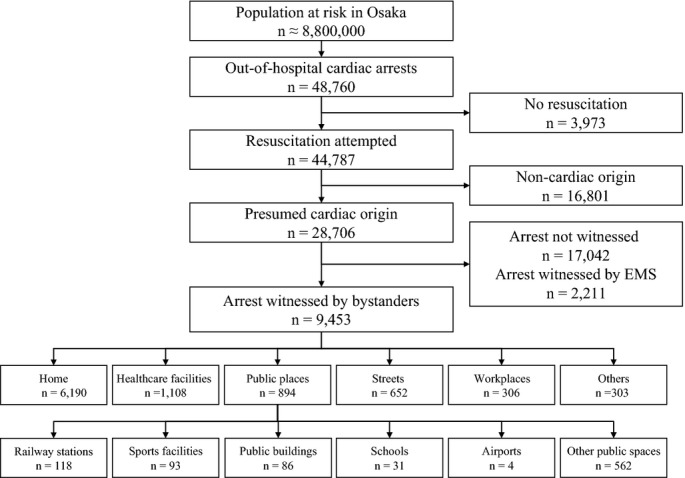
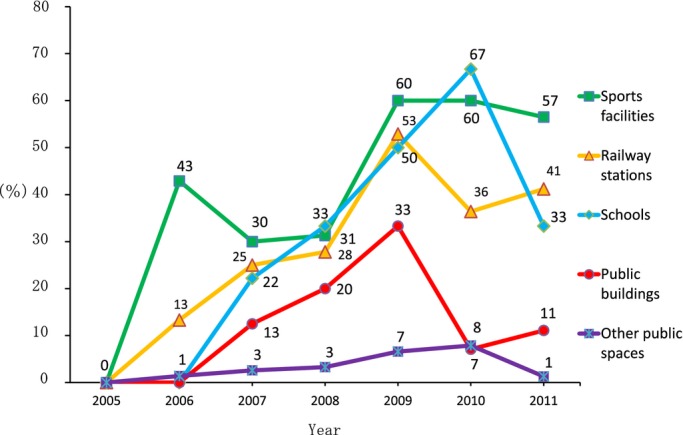
Methods and results: This, prospective, population-based observational study in Osaka, Japan, included consecutive out-of-hospital cardiac arrest (OHCA) patients with resuscitation attempts during 7 years, from January 2005 through December 2011. The trends in the proportion of public-access AED use and 1-month survival with neurologically favorable outcome were evaluated by location. Factors associated with neurologically favorable outcome (defined as cerebral performance category 1 or 2) after ventricular fibrillation were also assessed using multiple logistic regression analysis. A total of 9453 bystander-witnessed OHCAs of cardiac origin were documented and 894 (9.5%) of them occurred at public places. The proportion of public-access AED use significantly increased from 0.0% (0/20) in 2005 to 41.2% (7/17) in 2011 at railway stations and from 0.0% (0/7) to 56.5% (13/23) at sports facilities. Mean time from collapse to shock was 5.0 minutes among those who received shocks with public-access AEDs. The proportion of neurologically favorable outcome was 28.0% (33/118) at railway stations, 51.6% (48/93) at sports facilities, 23.3% (20/86) in public buildings, and 41.9% (13/31) in schools. In multivariate analysis, early defibrillation, irrespective of bystander or emergency medical service (EMS) personnel, was significantly associated with neurologically favorable outcome (adjusted odds ratio for 1-minute increment, 0.89; 95% confidence interval, 0.87 to 0.92).
Conclusions: This large, population-based OHCA registry demonstrated that earlier shock, irrespective the shock provider (bystander or EMS personnel), contributed to improving outcome, and a public-access defibrillation program was successfully implemented so that shocks with public-access AEDs were delivered to over 40% of bystander-witnessed OHCAs and time to shock was shortened in some kinds of public places.
Keywords: automated external defibrillator; cardiac arrest; cardiopulmonary resuscitation; death, sudden; epidemiology.
Figures
Comment in
-
Cardiopulmonary resuscitation and public access defibrillation in the current era--can we do better yet?J Am Heart Assoc. 2014 Apr 23;3(2):e000945. doi: 10.1161/JAHA.114.000945. J Am Heart Assoc. 2014. PMID: 24760964 Free PMC article. No abstract available.
References
-
- 2010 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2010; 122:S250-S605 - PubMed
-
- Ambulance Service Planning Office of Fire and Disaster Management Agency of Japan. Effect of first aid for cardiopulmonary arrest Availbale at: http://www.fdma.go.jp/neuter/topics/kyukyukyujo_genkyo/h24/01_kyukyu.pdf. Accessed May 07, 2013 (in Japanese).
-
- 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010; 122:S639-S946 - PubMed
-
- European resuscitation council guidelines for resuscitation 2010. Resuscitation. 2010; 81:1219-1451 - PubMed
-
- 2010 Japanese Guidelines for Emergency Care and Cardiopulmonary Resuscitation. 20111st edTokyo: Health Shuppansha
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
